{"title":"Noninvasive early identification of durable clinical benefit from immune checkpoint inhibition: a prospective multicenter study (NCT04566432)","authors":"Xinghao Ai, Bo Jia, Zhiyi He, Junping Zhang, Minglei Zhuo, Jun Zhao, Zhe Wang, Jiexia Zhang, Zaiwen Fan, Xiaotong Zhang, Chong Li, Feng Jin, Ziming Li, Xia Ma, Hao Tang, Xiang Yan, Wei Li, Yuanyuan Xiong, Huan Yin, Rongrong Chen, Shun Lu","doi":"10.1038/s41392-024-02060-3","DOIUrl":null,"url":null,"abstract":"<p>Immune checkpoint inhibitors (ICIs) have changed the treatment landscape for patients with non-small cell lung cancer (NSCLC). In spite of durable responses in some patients, many patients develop early disease progression during the ICI treatment. Thus, early identification of patients with no durable benefit would facilitate the clinical decision for these patients. In this prospective, multicenter study, 101 non-<i>EGFR/ALK</i> patients who received ICI treatment were enrolled after screening 328 stage III-IV NSCLC patients. At the date of cutoff, 83 patients were eligible for ICI efficacy evaluation, with 56 patients having progress-free survival (PFS) over 6 months, which was defined as durable clinical benefit (DCB). A multimodal model was established by integrating normalized bTMB, early dynamic of ctDNA and the first RECIST response. This model could robustly predict DCB with area under the curve (AUC) of 0.878, sensitivity of 79.2% at 86.4% specificity (accuracy = 80.0%). This model was further validated in the independent cohort of the DIREct-On study with AUC of 0.887, sensitivity of 94.7% at 85.3% specificity (accuracy = 90.3%). Patients with higher predict scores had substantially longer PFS than those with lower scores (training cohort: median PFS 13.6 vs 4.2 months, <i>P</i> < 0.001, HR = 0.24; validation cohort: median PFS 11.0 vs 2.2 months, <i>P</i> < 0.001, HR = 0.17). Taken together, these results demonstrate that integrating early changes of ctDNA, normalized bTMB, and the first RECIST response can provide accurate, noninvasive, and early prediction of durable benefits for NSCLC patients treated with ICIs. Further prospective studies are warranted to validate these findings and guide clinical decision-making for optimal immunotherapy in NSCLC patients.</p>","PeriodicalId":21766,"journal":{"name":"Signal Transduction and Targeted Therapy","volume":"38 1","pages":""},"PeriodicalIF":52.7000,"publicationDate":"2024-12-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Signal Transduction and Targeted Therapy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1038/s41392-024-02060-3","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"BIOCHEMISTRY & MOLECULAR BIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
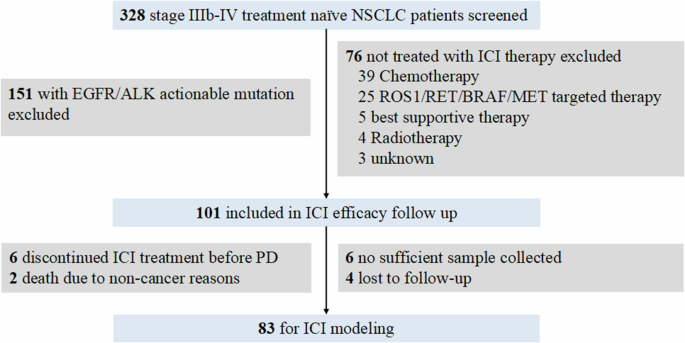
Immune checkpoint inhibitors (ICIs) have changed the treatment landscape for patients with non-small cell lung cancer (NSCLC). In spite of durable responses in some patients, many patients develop early disease progression during the ICI treatment. Thus, early identification of patients with no durable benefit would facilitate the clinical decision for these patients. In this prospective, multicenter study, 101 non-EGFR/ALK patients who received ICI treatment were enrolled after screening 328 stage III-IV NSCLC patients. At the date of cutoff, 83 patients were eligible for ICI efficacy evaluation, with 56 patients having progress-free survival (PFS) over 6 months, which was defined as durable clinical benefit (DCB). A multimodal model was established by integrating normalized bTMB, early dynamic of ctDNA and the first RECIST response. This model could robustly predict DCB with area under the curve (AUC) of 0.878, sensitivity of 79.2% at 86.4% specificity (accuracy = 80.0%). This model was further validated in the independent cohort of the DIREct-On study with AUC of 0.887, sensitivity of 94.7% at 85.3% specificity (accuracy = 90.3%). Patients with higher predict scores had substantially longer PFS than those with lower scores (training cohort: median PFS 13.6 vs 4.2 months, P < 0.001, HR = 0.24; validation cohort: median PFS 11.0 vs 2.2 months, P < 0.001, HR = 0.17). Taken together, these results demonstrate that integrating early changes of ctDNA, normalized bTMB, and the first RECIST response can provide accurate, noninvasive, and early prediction of durable benefits for NSCLC patients treated with ICIs. Further prospective studies are warranted to validate these findings and guide clinical decision-making for optimal immunotherapy in NSCLC patients.
期刊介绍:
Signal Transduction and Targeted Therapy is an open access journal that focuses on timely publication of cutting-edge discoveries and advancements in basic science and clinical research related to signal transduction and targeted therapy.
Scope: The journal covers research on major human diseases, including, but not limited to:
Cancer,Cardiovascular diseases,Autoimmune diseases,Nervous system diseases.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
