Comparative Safety of Istradefylline Among Parkinson Disease Adjunctive Therapies: A Systematic Review and Meta-analysis of Randomized Controlled Studies.
Yasar Torres-Yaghi, Joyce Qian, Hannah Cummings, Hiroo Shimoda, Satoru Ito, Sarah Batson, Stephen Mitchell, Fernando Pagan
{"title":"Comparative Safety of Istradefylline Among Parkinson Disease Adjunctive Therapies: A Systematic Review and Meta-analysis of Randomized Controlled Studies.","authors":"Yasar Torres-Yaghi, Joyce Qian, Hannah Cummings, Hiroo Shimoda, Satoru Ito, Sarah Batson, Stephen Mitchell, Fernando Pagan","doi":"10.1097/WNF.0000000000000620","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Adjunctive therapies to treat OFF episodes resulting from long-term levodopa treatment in Parkinson disease (PD) are hampered by safety and tolerability issues. Istradefylline offers an alternative mechanism (adenosine A2A receptor antagonist) and therefore potentially improved tolerability.</p><p><strong>Methods: </strong>A systematic review of PD adjuncts published in 2011 was updated to include randomized controlled trials published from January 1, 2010-April 15, 2019. Pairwise meta-analyses were updated, and Bucher indirect comparisons were used to generate estimates of relative safety, presented as odds ratio (OR) and 95% confidence interval (CI) for comparators versus istradefylline.</p><p><strong>Results: </strong>Fifty-seven randomized controlled trials involving 11,517 patients were included in the meta-analysis. Relative to istradefylline, dopamine agonists and catechol-O-methyl transferase (COMT) inhibitors had statistically significant higher odds of dyskinesia and somnolence. Monoamine oxidase-B inhibitors had significantly higher odds of hypotension. Amantadine extended-release (ER) had statistically significant higher odds of hallucination, orthostatic hypotension, insomnia, and withdrawals due to adverse events. All interventions combined had significantly higher odds of dyskinesia versus istradefylline 20 mg and somnolence versus istradefylline 40 mg. Considering overall incidence of adverse events, COMT inhibitors and amantadine ER had statistically significant higher odds versus both istradefylline doses (COMT versus istradefylline 40 mg, OR: 1.33; 95% CI: 1.03, 1.75; versus istradefylline 20 mg, OR: 1.32; 95% CI: 1.01, 1.72; amantadine ER versus istradefylline 40 mg, OR: 3.45; 95% CI: 1.85, 6.25; versus istradefylline 20 mg, OR: 3.33; 95% CI: 1.82, 6.25).</p><p><strong>Conclusion: </strong>Istradefylline was associated with a generally favorable safety profile relative to other adjunct medications in this study.</p>","PeriodicalId":10449,"journal":{"name":"Clinical Neuropharmacology","volume":"48 1","pages":"7-12"},"PeriodicalIF":1.5000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11913241/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Neuropharmacology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1097/WNF.0000000000000620","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Adjunctive therapies to treat OFF episodes resulting from long-term levodopa treatment in Parkinson disease (PD) are hampered by safety and tolerability issues. Istradefylline offers an alternative mechanism (adenosine A2A receptor antagonist) and therefore potentially improved tolerability.
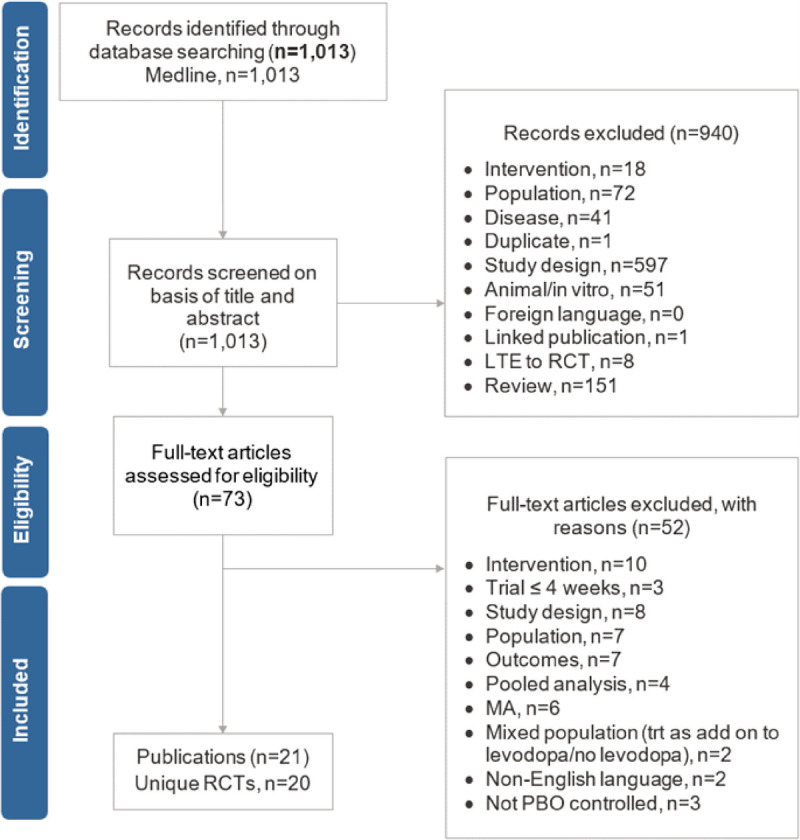
Methods: A systematic review of PD adjuncts published in 2011 was updated to include randomized controlled trials published from January 1, 2010-April 15, 2019. Pairwise meta-analyses were updated, and Bucher indirect comparisons were used to generate estimates of relative safety, presented as odds ratio (OR) and 95% confidence interval (CI) for comparators versus istradefylline.
Results: Fifty-seven randomized controlled trials involving 11,517 patients were included in the meta-analysis. Relative to istradefylline, dopamine agonists and catechol-O-methyl transferase (COMT) inhibitors had statistically significant higher odds of dyskinesia and somnolence. Monoamine oxidase-B inhibitors had significantly higher odds of hypotension. Amantadine extended-release (ER) had statistically significant higher odds of hallucination, orthostatic hypotension, insomnia, and withdrawals due to adverse events. All interventions combined had significantly higher odds of dyskinesia versus istradefylline 20 mg and somnolence versus istradefylline 40 mg. Considering overall incidence of adverse events, COMT inhibitors and amantadine ER had statistically significant higher odds versus both istradefylline doses (COMT versus istradefylline 40 mg, OR: 1.33; 95% CI: 1.03, 1.75; versus istradefylline 20 mg, OR: 1.32; 95% CI: 1.01, 1.72; amantadine ER versus istradefylline 40 mg, OR: 3.45; 95% CI: 1.85, 6.25; versus istradefylline 20 mg, OR: 3.33; 95% CI: 1.82, 6.25).
Conclusion: Istradefylline was associated with a generally favorable safety profile relative to other adjunct medications in this study.
期刊介绍:
Clinical Neuropharmacology is a peer-reviewed journal devoted to the pharmacology of the nervous system in its broadest sense. Coverage ranges from such basic aspects as mechanisms of action, structure-activity relationships, and drug metabolism and pharmacokinetics, to practical clinical problems such as drug interactions, drug toxicity, and therapy for specific syndromes and symptoms. The journal publishes original articles and brief reports, invited and submitted reviews, and letters to the editor. A regular feature is the Patient Management Series: in-depth case presentations with clinical questions and answers.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
