Jessica Cruttenden MD , Christopher Weil MD , Danae Byer BS , Lindsay Burt MD , Gita Suneja MD , David Gaffney MD, PhD , Cristina DeCesaris MD
{"title":"Patterns of Care in Adjuvant Radiation Therapy for Stage II Endometrioid Endometrial Adenocarcinoma: A National Cancer Database Analysis","authors":"Jessica Cruttenden MD , Christopher Weil MD , Danae Byer BS , Lindsay Burt MD , Gita Suneja MD , David Gaffney MD, PhD , Cristina DeCesaris MD","doi":"10.1016/j.adro.2024.101698","DOIUrl":null,"url":null,"abstract":"<div><h3>Purpose</h3><div>Treating stage II endometrial cancer involves total hysterectomy, bilateral salpingo-oophorectomy, and risk-adapted adjuvant therapy. Professional guidelines support various adjuvant treatments, but high-level data supporting specific options are conflicting. We sought to evaluate adjuvant radiation therapy (RT) trends for these patients, hypothesizing increased utilization of pelvic external beam RT (EBRT) over time.</div></div><div><h3>Methods and Materials</h3><div>Patients diagnosed in 2004-2019 with stage II endometrioid endometrial cancer who underwent total hysterectomy, bilateral salpingo-oophorectomy, and surgical staging were identified in the National Cancer Database. Patient characteristics per adjuvant RT received were compared using Wilcoxon rank sum and analysis of variance testing. Multivariable regression analysis (MVA) identified variables associated with EBRT, vaginal brachytherapy (VBT), or RT omission. A <em>P</em> value < .05 was significant, except in MVA, where Bonferroni correction was employed (<em>p</em> value < .017).</div></div><div><h3>Results</h3><div>Patients meeting criteria totaled 18,798; 19% received adjuvant EBRT alone, 25% VBT alone, 24% EBRT + VBT, and 32% no RT. Adjuvant RT use increased from 2004 to 2019, particularly EBRT + VBT (<em>p</em> < .05). In MVA, community hospital treatment (odds ratio [OR], 1.8; <em>p</em> < .001), Midwest location (OR, 1.2; <em>p</em> = .02), single-agent chemotherapy receipt (OR, 6.9; <em>p</em> < .001), lymphovascular space invasion (OR, 1.4; <em>p</em> < .001), and positive surgical margins (OR, 1.8; <em>p</em> < .001) were positively associated with EBRT. No variables were positively associated with VBT. Black race (OR, 1.2; <em>p</em> = .03), community hospital treatment (OR, 1.4; <em>p</em> = .04), South (OR, 2.2; <em>p</em> < .001) or West (OR, 2.1; <em>p</em> < .001) location, distance >50 miles from the treatment center (OR, 1.5; <em>p</em> < .001), and grade 2 (OR, 1.2; <em>p</em> < .001) or 3 (OR, 1.3; <em>p</em> = .01) disease were associated with RT omission.</div></div><div><h3>Conclusions</h3><div>Adjuvant RT for stage II endometrial cancer increased over time, particularly EBRT + VBT. Patient-related factors such as race, region, and distance from the treatment center were associated with RT omission, suggesting sociodemographic barriers to care. Tumor-related factors such as positive surgical margins and lymphovascular space invasion were associated with EBRT receipt, suggesting consideration of high-risk factors for locoregional recurrence in adjuvant RT approaches.</div></div>","PeriodicalId":7390,"journal":{"name":"Advances in Radiation Oncology","volume":"10 2","pages":"Article 101698"},"PeriodicalIF":2.7000,"publicationDate":"2025-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11730229/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Advances in Radiation Oncology","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2452109424002616","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/3 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose
Treating stage II endometrial cancer involves total hysterectomy, bilateral salpingo-oophorectomy, and risk-adapted adjuvant therapy. Professional guidelines support various adjuvant treatments, but high-level data supporting specific options are conflicting. We sought to evaluate adjuvant radiation therapy (RT) trends for these patients, hypothesizing increased utilization of pelvic external beam RT (EBRT) over time.
Methods and Materials
Patients diagnosed in 2004-2019 with stage II endometrioid endometrial cancer who underwent total hysterectomy, bilateral salpingo-oophorectomy, and surgical staging were identified in the National Cancer Database. Patient characteristics per adjuvant RT received were compared using Wilcoxon rank sum and analysis of variance testing. Multivariable regression analysis (MVA) identified variables associated with EBRT, vaginal brachytherapy (VBT), or RT omission. A P value < .05 was significant, except in MVA, where Bonferroni correction was employed (p value < .017).
Results
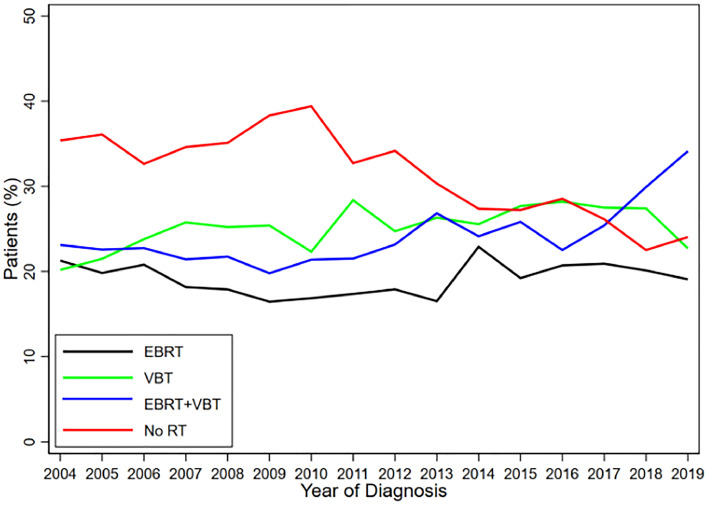
Patients meeting criteria totaled 18,798; 19% received adjuvant EBRT alone, 25% VBT alone, 24% EBRT + VBT, and 32% no RT. Adjuvant RT use increased from 2004 to 2019, particularly EBRT + VBT (p < .05). In MVA, community hospital treatment (odds ratio [OR], 1.8; p < .001), Midwest location (OR, 1.2; p = .02), single-agent chemotherapy receipt (OR, 6.9; p < .001), lymphovascular space invasion (OR, 1.4; p < .001), and positive surgical margins (OR, 1.8; p < .001) were positively associated with EBRT. No variables were positively associated with VBT. Black race (OR, 1.2; p = .03), community hospital treatment (OR, 1.4; p = .04), South (OR, 2.2; p < .001) or West (OR, 2.1; p < .001) location, distance >50 miles from the treatment center (OR, 1.5; p < .001), and grade 2 (OR, 1.2; p < .001) or 3 (OR, 1.3; p = .01) disease were associated with RT omission.
Conclusions
Adjuvant RT for stage II endometrial cancer increased over time, particularly EBRT + VBT. Patient-related factors such as race, region, and distance from the treatment center were associated with RT omission, suggesting sociodemographic barriers to care. Tumor-related factors such as positive surgical margins and lymphovascular space invasion were associated with EBRT receipt, suggesting consideration of high-risk factors for locoregional recurrence in adjuvant RT approaches.
期刊介绍:
The purpose of Advances is to provide information for clinicians who use radiation therapy by publishing: Clinical trial reports and reanalyses. Basic science original reports. Manuscripts examining health services research, comparative and cost effectiveness research, and systematic reviews. Case reports documenting unusual problems and solutions. High quality multi and single institutional series, as well as other novel retrospective hypothesis generating series. Timely critical reviews on important topics in radiation oncology, such as side effects. Articles reporting the natural history of disease and patterns of failure, particularly as they relate to treatment volume delineation. Articles on safety and quality in radiation therapy. Essays on clinical experience. Articles on practice transformation in radiation oncology, in particular: Aspects of health policy that may impact the future practice of radiation oncology. How information technology, such as data analytics and systems innovations, will change radiation oncology practice. Articles on imaging as they relate to radiation therapy treatment.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
