Fatima Cardoso, Joyce O’Shaughnessy, Zhenzhen Liu, Heather McArthur, Peter Schmid, Javier Cortes, Nadia Harbeck, Melinda L. Telli, David W. Cescon, Peter A. Fasching, Zhimin Shao, Delphine Loirat, Yeon Hee Park, Manuel Gonzalez Fernandez, Gábor Rubovszky, Laura Spring, Seock-Ah Im, Rina Hui, Toshimi Takano, Fabrice André, Hiroyuki Yasojima, Yu Ding, Liyi Jia, Vassiliki Karantza, Konstantinos Tryfonidis, Aditya Bardia
{"title":"Pembrolizumab and chemotherapy in high-risk, early-stage, ER+/HER2− breast cancer: a randomized phase 3 trial","authors":"Fatima Cardoso, Joyce O’Shaughnessy, Zhenzhen Liu, Heather McArthur, Peter Schmid, Javier Cortes, Nadia Harbeck, Melinda L. Telli, David W. Cescon, Peter A. Fasching, Zhimin Shao, Delphine Loirat, Yeon Hee Park, Manuel Gonzalez Fernandez, Gábor Rubovszky, Laura Spring, Seock-Ah Im, Rina Hui, Toshimi Takano, Fabrice André, Hiroyuki Yasojima, Yu Ding, Liyi Jia, Vassiliki Karantza, Konstantinos Tryfonidis, Aditya Bardia","doi":"10.1038/s41591-024-03415-7","DOIUrl":null,"url":null,"abstract":"Addition of pembrolizumab to neoadjuvant chemotherapy followed by adjuvant pembrolizumab improved outcomes in patients with high-risk, early-stage, triple-negative breast cancer. However, whether the addition of neoadjuvant pembrolizumab to chemotherapy would improve outcomes in high-risk, early-stage, estrogen receptor-positive/human epidermal growth factor receptor 2-negative (ER+/HER2−) breast cancer remains unclear. We conducted a double-blind, placebo-controlled phase 3 study (KEYNOTE-756) in which patients with previously untreated ER+/HER2− grade 3 high-risk invasive breast cancer (T1c-2 (≥2 cm), cN1–2 or T3–4, cN0–2) were randomly assigned (1:1) to neoadjuvant pembrolizumab 200 mg or placebo Q3W given with paclitaxel QW for 12 weeks, followed by four cycles of doxorubicin or epirubicin plus cyclophosphamide Q2W or Q3W. After surgery (with/without adjuvant radiation therapy), patients received adjuvant pembrolizumab or placebo for nine cycles plus adjuvant endocrine therapy. Dual primary endpoints were pathological complete response and event-free survival in the intention-to-treat population. In total, 635 patients were assigned to the pembrolizumab−chemotherapy arm and 643 to the placebo−chemotherapy arm. At the study’s prespecified first interim analysis, the pathological complete response rate was 24.3% (95% confidence interval (CI), 21.0–27.8%) in the pembrolizumab−chemotherapy arm and 15.6% (95% CI, 12.8–18.6%) in the placebo−chemotherapy arm (estimated treatment difference, 8.5 percentage points; 95% CI, 4.2–12.8; P = 0.00005). Event-free survival was not mature in this analysis. During the neoadjuvant phase, treatment-related adverse events of grade ≥3 were reported in 52.5% and 46.4% of patients in the pembrolizumab−chemotherapy and placebo−chemotherapy arms, respectively. In summary, the addition of pembrolizumab to neoadjuvant chemotherapy significantly improved the pathological complete response rate in patients with high-risk, early-stage ER+/HER2− breast cancer. Safety was consistent with the known profiles of each study treatment. Follow-up continues for event-free survival. ClinicalTrials.gov identifier: NCT03725059 . In this prespecified interim analysis of the KEYNOTE-756 phase 3 trial, pembrolizumab and chemotherapy treatment of patients with high-risk, early-stage, estrogen receptor-positive/human epidermal growth factor receptor-negative breast cancer improved the pathological complete response rate compared with chemotherapy alone.","PeriodicalId":19037,"journal":{"name":"Nature Medicine","volume":"31 2","pages":"442-448"},"PeriodicalIF":50.0000,"publicationDate":"2025-01-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.nature.com/articles/s41591-024-03415-7.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Nature Medicine","FirstCategoryId":"3","ListUrlMain":"https://www.nature.com/articles/s41591-024-03415-7","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"BIOCHEMISTRY & MOLECULAR BIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
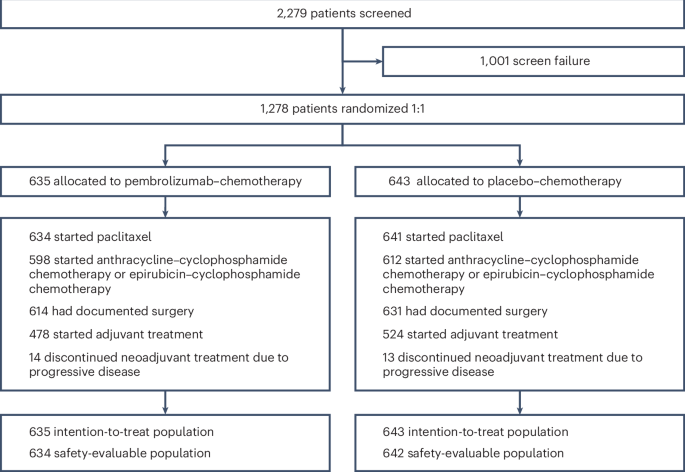
Addition of pembrolizumab to neoadjuvant chemotherapy followed by adjuvant pembrolizumab improved outcomes in patients with high-risk, early-stage, triple-negative breast cancer. However, whether the addition of neoadjuvant pembrolizumab to chemotherapy would improve outcomes in high-risk, early-stage, estrogen receptor-positive/human epidermal growth factor receptor 2-negative (ER+/HER2−) breast cancer remains unclear. We conducted a double-blind, placebo-controlled phase 3 study (KEYNOTE-756) in which patients with previously untreated ER+/HER2− grade 3 high-risk invasive breast cancer (T1c-2 (≥2 cm), cN1–2 or T3–4, cN0–2) were randomly assigned (1:1) to neoadjuvant pembrolizumab 200 mg or placebo Q3W given with paclitaxel QW for 12 weeks, followed by four cycles of doxorubicin or epirubicin plus cyclophosphamide Q2W or Q3W. After surgery (with/without adjuvant radiation therapy), patients received adjuvant pembrolizumab or placebo for nine cycles plus adjuvant endocrine therapy. Dual primary endpoints were pathological complete response and event-free survival in the intention-to-treat population. In total, 635 patients were assigned to the pembrolizumab−chemotherapy arm and 643 to the placebo−chemotherapy arm. At the study’s prespecified first interim analysis, the pathological complete response rate was 24.3% (95% confidence interval (CI), 21.0–27.8%) in the pembrolizumab−chemotherapy arm and 15.6% (95% CI, 12.8–18.6%) in the placebo−chemotherapy arm (estimated treatment difference, 8.5 percentage points; 95% CI, 4.2–12.8; P = 0.00005). Event-free survival was not mature in this analysis. During the neoadjuvant phase, treatment-related adverse events of grade ≥3 were reported in 52.5% and 46.4% of patients in the pembrolizumab−chemotherapy and placebo−chemotherapy arms, respectively. In summary, the addition of pembrolizumab to neoadjuvant chemotherapy significantly improved the pathological complete response rate in patients with high-risk, early-stage ER+/HER2− breast cancer. Safety was consistent with the known profiles of each study treatment. Follow-up continues for event-free survival. ClinicalTrials.gov identifier: NCT03725059 . In this prespecified interim analysis of the KEYNOTE-756 phase 3 trial, pembrolizumab and chemotherapy treatment of patients with high-risk, early-stage, estrogen receptor-positive/human epidermal growth factor receptor-negative breast cancer improved the pathological complete response rate compared with chemotherapy alone.
期刊介绍:
Nature Medicine is a monthly journal publishing original peer-reviewed research in all areas of medicine. The publication focuses on originality, timeliness, interdisciplinary interest, and the impact on improving human health. In addition to research articles, Nature Medicine also publishes commissioned content such as News, Reviews, and Perspectives. This content aims to provide context for the latest advances in translational and clinical research, reaching a wide audience of M.D. and Ph.D. readers. All editorial decisions for the journal are made by a team of full-time professional editors.
Nature Medicine consider all types of clinical research, including:
-Case-reports and small case series
-Clinical trials, whether phase 1, 2, 3 or 4
-Observational studies
-Meta-analyses
-Biomarker studies
-Public and global health studies
Nature Medicine is also committed to facilitating communication between translational and clinical researchers. As such, we consider “hybrid” studies with preclinical and translational findings reported alongside data from clinical studies.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
