Idnan Yunas, Ioannis D Gallos, Adam J Devall, Marcelina Podesek, John Allotey, Yemisi Takwoingi, Arri Coomarasamy
{"title":"Tests for diagnosis of postpartum haemorrhage at vaginal birth.","authors":"Idnan Yunas, Ioannis D Gallos, Adam J Devall, Marcelina Podesek, John Allotey, Yemisi Takwoingi, Arri Coomarasamy","doi":"10.1002/14651858.CD016134","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Postpartum haemorrhage (PPH) is the leading cause of maternal mortality worldwide. Accurate diagnosis of PPH can prevent adverse outcomes by enabling early treatment.</p><p><strong>Objectives: </strong>What is the accuracy of methods (index tests) for diagnosing primary PPH (blood loss ≥ 500 mL in the first 24 hours after birth) and severe primary PPH (blood loss ≥ 1000 mL in the first 24 hours after birth) (target conditions) in women giving birth vaginally (participants) compared to weighed blood loss measurement or other objective measurements of blood loss (reference standards)?</p><p><strong>Search methods: </strong>We searched CENTRAL, MEDLINE, Embase, Web of Science Core Collection, ClinicalTrials.gov, and the World Health Organization International Clinical Trials Registry Platform to 24 May 2024.</p><p><strong>Selection criteria: </strong>We included women who gave birth vaginally in any setting. Study types included diagnostic cohort studies and cross-sectional studies that reported 2 x 2 data (number of true positive, false positive, false negative, and true negative results) or where the 2 x 2 data could be derived from test accuracy estimates. Eligible index tests included: visual estimation; calibrated blood collection devices; approach with calibrated drape and observations; blood loss estimation using the SAPHE (Signalling a Postpartum Hemorrhage Emergency) Mat; blood loss field image analysis and other technologies; uterine atony assessment; clinical variables (e.g. heart rate, blood pressure, shock index); early warning charts; haemoglobin levels; and predelivery fibrinogen levels. Eligible reference standards included objective methods such as: gravimetric blood loss measurement, which involves weighing collected blood, as well as weighing blood-soaked pads, gauze and sheets, and subtracting their dry weight; calibrated devices to measure blood volume (volumetric blood loss measurement); the alkaline-haematin method of blood loss estimation; and blood extracted using machine-extraction and measured spectrometrically as oxyhaemoglobin.</p><p><strong>Data collection and analysis: </strong>At least two review authors, working independently, undertook study screening, selection, data extraction, assessment of risk of bias, and assessment of the certainty of the evidence. We resolved any differences through consensus or with input from another author. We generated 2 x 2 tables of the true positives, true negatives, false positives, and false negatives to calculate the sensitivity, specificity, and 95% confidence intervals for each index test. We presented sensitivity and specificity estimates from studies in forest plots. Where possible, we conducted meta-analyses for each index test and reference standard combination for each target condition. We examined heterogeneity by visual inspection of the forest plots.</p><p><strong>Main results: </strong>Our review included 18 studies with a total of 291,040 participants. Fourteen studies evaluated PPH and seven studies evaluated severe PPH. Most studies were conducted in a hospital setting (16 of 18). There were four studies at high risk of bias for the patient selection domain and 14 studies at low risk. For the index test domain, 10 studies were at low risk of bias, seven studies at high risk, and one study at uncertain risk. For the reference standard domain, one study was at high risk of bias and 17 studies at low risk. For the flow and timing domain, three studies were at high risk of bias and 15 studies at low risk. The applicability concerns were low for all studies across the domains. In the abstract, we have prioritised reporting results for common, important thresholds for index tests or where the certainty of the evidence for the sensitivity estimate was at least moderate. Full results are in the main body of the review. PPH (blood loss ≥ 500 mL) For PPH, visual estimation with gravimetric blood loss measurement as the reference standard had 48% sensitivity (95% confidence interval (CI) 44% to 53%; moderate certainty) and 97% specificity (95% CI 95% to 99%; high certainty) (4 studies, 196,305 participants). Visual estimation with volumetric blood loss measurement as the reference standard showed 22% sensitivity (95% CI 12% to 37%; moderate certainty) and 99% specificity (95% CI 97% to 100%; moderate certainty) (2 studies, 514 participants). The diagnostic approach with calibrated drape plus observations, with gravimetric blood loss measurement as the reference standard for PPH, showed 93% sensitivity (95% CI 92% to 94%; high certainty) and 95% specificity (95% CI 95% to 96%; high certainty) (2 studies, 53,762 participants). A haemoglobin level of less than 10 g/dL with gravimetric blood loss measurement as the reference standard showed 37% sensitivity (95% CI 30% to 44%; high certainty) and 79% specificity (95% CI 76% to 82%; high certainty) (1 study, 1058 participants). Severe PPH (blood loss ≥ 1000 mL) For severe PPH, visual estimation, with volumetric plus gravimetric blood loss measurement as the reference standard, showed 9% sensitivity (95% CI 0% to 41%; low certainty) and 100% specificity (95% CI 99% to 100%; moderate certainty) (1 study, 274 participants). A shock index level of 1.0 or higher (commonly used as a threshold for severe PPH) up to two hours after birth, with gravimetric blood loss measurement as the reference standard, showed 30% sensitivity (95% CI 27% to 33%; moderate certainty) and 93% specificity (95% CI 92% to 93%; moderate certainty) (1 study, 30,820 participants). A haemoglobin level of less than 10 g/dL, with gravimetric blood loss measurement as the reference standard, showed 71% sensitivity (95% CI 51% to 87%; moderate certainty) and 77% specificity (95% CI 75% to 80%; high certainty) (1 study, 1058 participants).</p><p><strong>Authors' conclusions: </strong>Visual estimation of blood loss to diagnose PPH showed low sensitivity and is likely to miss the diagnosis in half of women giving birth vaginally. A diagnostic approach using a calibrated drape to objectively measure blood loss plus clinical observations showed high sensitivity and specificity for diagnosing PPH. Other index tests showed low to moderate sensitivities in diagnosing PPH and severe PPH. Future research should determine the accuracy of diagnostic tests in non-hospital settings and consider combining index tests to increase the sensitivity of PPH diagnosis.</p><p><strong>Funding: </strong>Bill and Melinda Gates Foundation REGISTRATION: PROSPERO (CRD42024541874).</p>","PeriodicalId":10473,"journal":{"name":"Cochrane Database of Systematic Reviews","volume":"1 ","pages":"CD016134"},"PeriodicalIF":8.8000,"publicationDate":"2025-01-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11740288/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cochrane Database of Systematic Reviews","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1002/14651858.CD016134","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Postpartum haemorrhage (PPH) is the leading cause of maternal mortality worldwide. Accurate diagnosis of PPH can prevent adverse outcomes by enabling early treatment.
Objectives: What is the accuracy of methods (index tests) for diagnosing primary PPH (blood loss ≥ 500 mL in the first 24 hours after birth) and severe primary PPH (blood loss ≥ 1000 mL in the first 24 hours after birth) (target conditions) in women giving birth vaginally (participants) compared to weighed blood loss measurement or other objective measurements of blood loss (reference standards)?
Search methods: We searched CENTRAL, MEDLINE, Embase, Web of Science Core Collection, ClinicalTrials.gov, and the World Health Organization International Clinical Trials Registry Platform to 24 May 2024.
Selection criteria: We included women who gave birth vaginally in any setting. Study types included diagnostic cohort studies and cross-sectional studies that reported 2 x 2 data (number of true positive, false positive, false negative, and true negative results) or where the 2 x 2 data could be derived from test accuracy estimates. Eligible index tests included: visual estimation; calibrated blood collection devices; approach with calibrated drape and observations; blood loss estimation using the SAPHE (Signalling a Postpartum Hemorrhage Emergency) Mat; blood loss field image analysis and other technologies; uterine atony assessment; clinical variables (e.g. heart rate, blood pressure, shock index); early warning charts; haemoglobin levels; and predelivery fibrinogen levels. Eligible reference standards included objective methods such as: gravimetric blood loss measurement, which involves weighing collected blood, as well as weighing blood-soaked pads, gauze and sheets, and subtracting their dry weight; calibrated devices to measure blood volume (volumetric blood loss measurement); the alkaline-haematin method of blood loss estimation; and blood extracted using machine-extraction and measured spectrometrically as oxyhaemoglobin.
Data collection and analysis: At least two review authors, working independently, undertook study screening, selection, data extraction, assessment of risk of bias, and assessment of the certainty of the evidence. We resolved any differences through consensus or with input from another author. We generated 2 x 2 tables of the true positives, true negatives, false positives, and false negatives to calculate the sensitivity, specificity, and 95% confidence intervals for each index test. We presented sensitivity and specificity estimates from studies in forest plots. Where possible, we conducted meta-analyses for each index test and reference standard combination for each target condition. We examined heterogeneity by visual inspection of the forest plots.
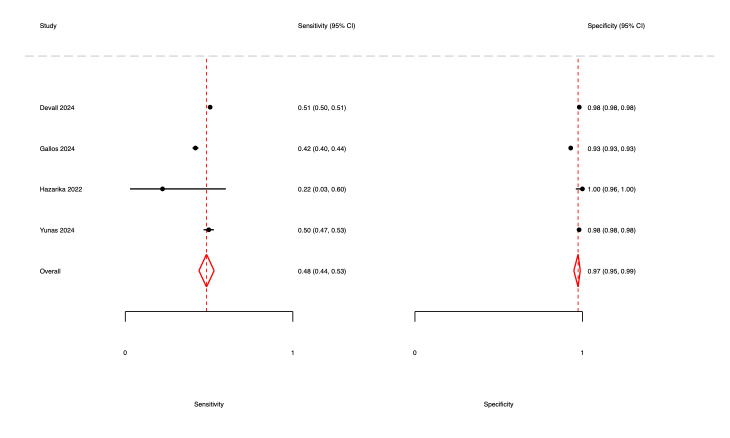
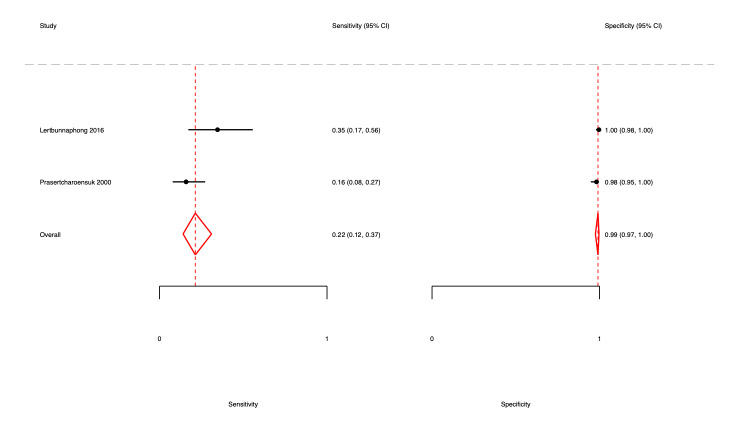
Main results: Our review included 18 studies with a total of 291,040 participants. Fourteen studies evaluated PPH and seven studies evaluated severe PPH. Most studies were conducted in a hospital setting (16 of 18). There were four studies at high risk of bias for the patient selection domain and 14 studies at low risk. For the index test domain, 10 studies were at low risk of bias, seven studies at high risk, and one study at uncertain risk. For the reference standard domain, one study was at high risk of bias and 17 studies at low risk. For the flow and timing domain, three studies were at high risk of bias and 15 studies at low risk. The applicability concerns were low for all studies across the domains. In the abstract, we have prioritised reporting results for common, important thresholds for index tests or where the certainty of the evidence for the sensitivity estimate was at least moderate. Full results are in the main body of the review. PPH (blood loss ≥ 500 mL) For PPH, visual estimation with gravimetric blood loss measurement as the reference standard had 48% sensitivity (95% confidence interval (CI) 44% to 53%; moderate certainty) and 97% specificity (95% CI 95% to 99%; high certainty) (4 studies, 196,305 participants). Visual estimation with volumetric blood loss measurement as the reference standard showed 22% sensitivity (95% CI 12% to 37%; moderate certainty) and 99% specificity (95% CI 97% to 100%; moderate certainty) (2 studies, 514 participants). The diagnostic approach with calibrated drape plus observations, with gravimetric blood loss measurement as the reference standard for PPH, showed 93% sensitivity (95% CI 92% to 94%; high certainty) and 95% specificity (95% CI 95% to 96%; high certainty) (2 studies, 53,762 participants). A haemoglobin level of less than 10 g/dL with gravimetric blood loss measurement as the reference standard showed 37% sensitivity (95% CI 30% to 44%; high certainty) and 79% specificity (95% CI 76% to 82%; high certainty) (1 study, 1058 participants). Severe PPH (blood loss ≥ 1000 mL) For severe PPH, visual estimation, with volumetric plus gravimetric blood loss measurement as the reference standard, showed 9% sensitivity (95% CI 0% to 41%; low certainty) and 100% specificity (95% CI 99% to 100%; moderate certainty) (1 study, 274 participants). A shock index level of 1.0 or higher (commonly used as a threshold for severe PPH) up to two hours after birth, with gravimetric blood loss measurement as the reference standard, showed 30% sensitivity (95% CI 27% to 33%; moderate certainty) and 93% specificity (95% CI 92% to 93%; moderate certainty) (1 study, 30,820 participants). A haemoglobin level of less than 10 g/dL, with gravimetric blood loss measurement as the reference standard, showed 71% sensitivity (95% CI 51% to 87%; moderate certainty) and 77% specificity (95% CI 75% to 80%; high certainty) (1 study, 1058 participants).
Authors' conclusions: Visual estimation of blood loss to diagnose PPH showed low sensitivity and is likely to miss the diagnosis in half of women giving birth vaginally. A diagnostic approach using a calibrated drape to objectively measure blood loss plus clinical observations showed high sensitivity and specificity for diagnosing PPH. Other index tests showed low to moderate sensitivities in diagnosing PPH and severe PPH. Future research should determine the accuracy of diagnostic tests in non-hospital settings and consider combining index tests to increase the sensitivity of PPH diagnosis.
Funding: Bill and Melinda Gates Foundation REGISTRATION: PROSPERO (CRD42024541874).
期刊介绍:
The Cochrane Database of Systematic Reviews (CDSR) stands as the premier database for systematic reviews in healthcare. It comprises Cochrane Reviews, along with protocols for these reviews, editorials, and supplements. Owned and operated by Cochrane, a worldwide independent network of healthcare stakeholders, the CDSR (ISSN 1469-493X) encompasses a broad spectrum of health-related topics, including health services.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
