Bjørk K Sofiudottir, Sören Möller, Robin Christensen, Stefan Harders, Grith L Sørensen, Jesper Blegvad, Mette Herly, Dzenan Masic, Grazina Urbonaviciene, Frank Andersen, Christin Isaksen, Brian Bridal Løgstrup, Charlotte Hyldgaard, Torkell Ellingsen
{"title":"Detecting respiratory impairment in newly diagnosed rheumatoid arthritis by MRC dyspnoea scale and microfibrillar-associated protein 4.","authors":"Bjørk K Sofiudottir, Sören Möller, Robin Christensen, Stefan Harders, Grith L Sørensen, Jesper Blegvad, Mette Herly, Dzenan Masic, Grazina Urbonaviciene, Frank Andersen, Christin Isaksen, Brian Bridal Løgstrup, Charlotte Hyldgaard, Torkell Ellingsen","doi":"10.1080/20018525.2024.2449270","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To evaluate the Medical Research Council (MRC) dyspnoea scale and serum Microfibrillar-associated protein 4 (MFAP4) levels for the detection of respiratory impairment in newly diagnosed rheumatoid arthritis (RA).</p><p><strong>Methods: </strong>Patients underwent blood tests, pulmonary function tests (PFT) and dyspnoea assessment using the MRC scale. Respiratory impairment was defined as a diffusion capacity of the lungs for carbon monoxide (DLCO) <80% predicted or FEV1/FVC <70%. The primary outcomes were the MRC and MFAP4's sensitivity, specificity, and diagnostic odds ratio (DOR) with 95% confidence intervals (CI).</p><p><strong>Results: </strong>One hundred and thirty-one patients had available baseline tests. Mean age was 57.7 years (SD: 10.9), 61% were female, and 45% had respiratory impairment. For MRC score ≥ 2, the sensitivity was 39.0% (95% CI 26.5; 52.6), specificity 76.4% (95% CI 64.9; 85.6), and DOR 2.07 (95% CI 0.97; 4.40). For MFAP4 > 29.0 U/mL, the sensitivity was 62.7% (95% CI 49.1; 75.0), specificity 56.9% (95% CI 44.7; 68.6), and DOR 2.22 (95% CI 1.10; 4.50). The DOR was 3.01 (95% CI 1.27; 7.16) for MFAP4 detecting respiratory impairment when adjusted for age, sex and smoking status.</p><p><strong>Conclusion: </strong>The MRC dyspnoea score and unadjusted MFAP4 levels were poor predictors of respiratory impairment in patients with early treatment-naïve rheumatoid arthritis.</p>","PeriodicalId":11872,"journal":{"name":"European Clinical Respiratory Journal","volume":"12 1","pages":"2449270"},"PeriodicalIF":1.4000,"publicationDate":"2025-01-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11749244/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Clinical Respiratory Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1080/20018525.2024.2449270","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: To evaluate the Medical Research Council (MRC) dyspnoea scale and serum Microfibrillar-associated protein 4 (MFAP4) levels for the detection of respiratory impairment in newly diagnosed rheumatoid arthritis (RA).
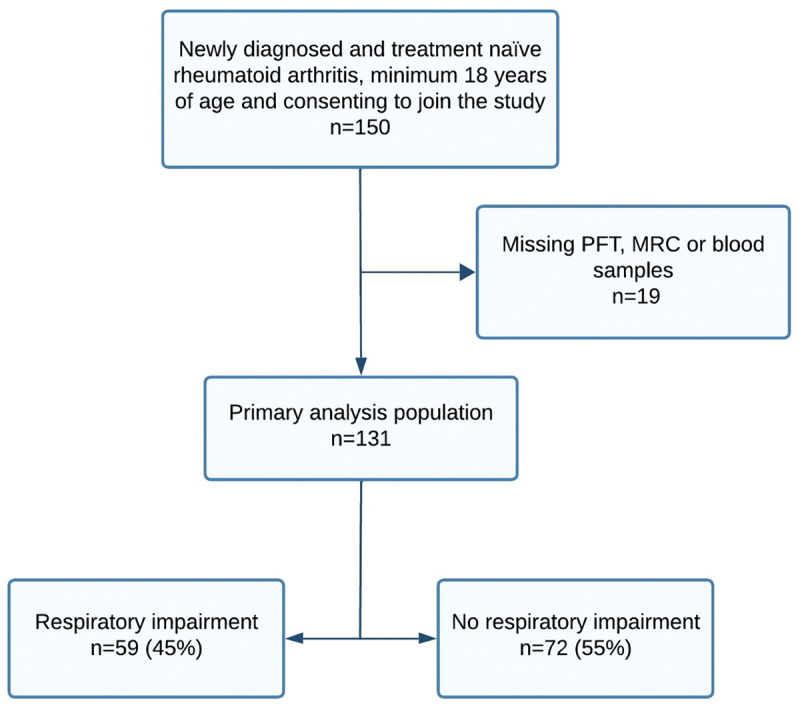
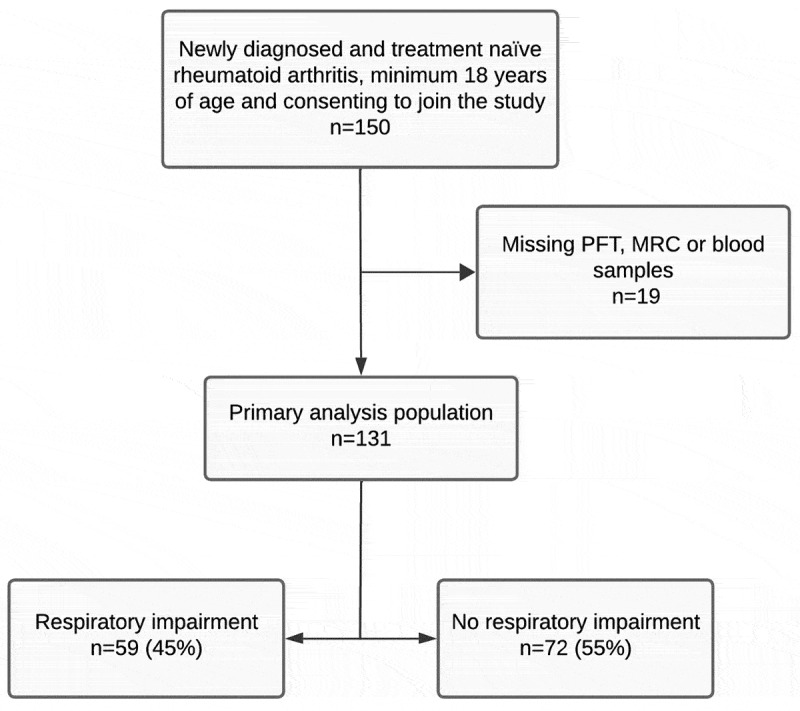
Methods: Patients underwent blood tests, pulmonary function tests (PFT) and dyspnoea assessment using the MRC scale. Respiratory impairment was defined as a diffusion capacity of the lungs for carbon monoxide (DLCO) <80% predicted or FEV1/FVC <70%. The primary outcomes were the MRC and MFAP4's sensitivity, specificity, and diagnostic odds ratio (DOR) with 95% confidence intervals (CI).
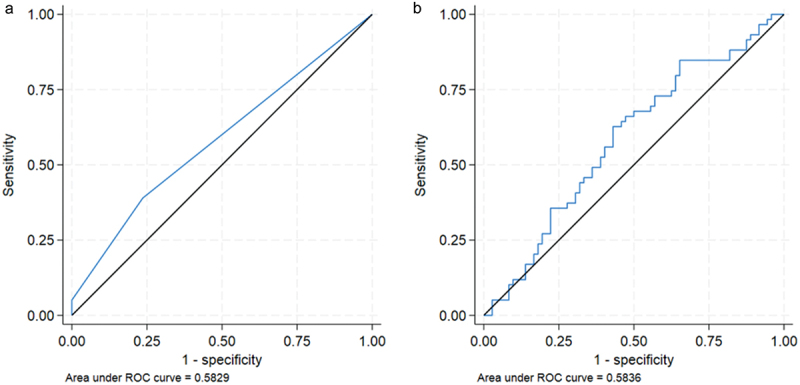
Results: One hundred and thirty-one patients had available baseline tests. Mean age was 57.7 years (SD: 10.9), 61% were female, and 45% had respiratory impairment. For MRC score ≥ 2, the sensitivity was 39.0% (95% CI 26.5; 52.6), specificity 76.4% (95% CI 64.9; 85.6), and DOR 2.07 (95% CI 0.97; 4.40). For MFAP4 > 29.0 U/mL, the sensitivity was 62.7% (95% CI 49.1; 75.0), specificity 56.9% (95% CI 44.7; 68.6), and DOR 2.22 (95% CI 1.10; 4.50). The DOR was 3.01 (95% CI 1.27; 7.16) for MFAP4 detecting respiratory impairment when adjusted for age, sex and smoking status.
Conclusion: The MRC dyspnoea score and unadjusted MFAP4 levels were poor predictors of respiratory impairment in patients with early treatment-naïve rheumatoid arthritis.
目的:评价医学研究委员会(MRC)呼吸困难量表和血清微纤维相关蛋白4 (MFAP4)水平在新诊断的类风湿关节炎(RA)中检测呼吸障碍的价值。方法:对患者进行血液检查、肺功能检查(PFT)和MRC评分评估呼吸困难。呼吸障碍被定义为肺对一氧化碳(DLCO)的扩散能力。结果:131例患者有可用的基线测试。平均年龄57.7岁(SD: 10.9), 61%为女性,45%为呼吸障碍。对于MRC评分≥2,敏感性为39.0% (95% CI 26.5;52.6),特异性76.4% (95% CI 64.9;85.6), DOR为2.07 (95% CI 0.97;4.40)。对于MFAP4 bb0 29.0 U/mL,敏感性为62.7% (95% CI 49.1;75.0),特异性56.9% (95% CI 44.7;68.6), DOR为2.22 (95% CI 1.10;4.50)。DOR为3.01 (95% CI 1.27;7.16) MFAP4在调整年龄、性别和吸烟状况后检测呼吸障碍。结论:MRC呼吸困难评分和未调整的MFAP4水平是早期treatment-naïve类风湿性关节炎患者呼吸功能障碍的不良预测指标。




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
