Henning Johann Steffen, Noah Abel, Felix Lau, Alexander Schmitt, Marielen Reinhardt, Muharrem Akin, Thomas Bertsch, Jonas Rusnak, Kathrin Weidner, Michael Behnes, Ibrahim Akin, Tobias Schupp
{"title":"Timing of acute decompensated heart failure in patients with heart failure and mildly reduced ejection fraction.","authors":"Henning Johann Steffen, Noah Abel, Felix Lau, Alexander Schmitt, Marielen Reinhardt, Muharrem Akin, Thomas Bertsch, Jonas Rusnak, Kathrin Weidner, Michael Behnes, Ibrahim Akin, Tobias Schupp","doi":"10.1007/s00380-024-02505-3","DOIUrl":null,"url":null,"abstract":"<p><p>This study investigates the prognosis of acute decompensated heart failure (ADHF) on admission (i.e., primary ADHF) as compared to ADHF onset during course of hospitalization (i.e., secondary ADHF) in patients hospitalized with heart failure with mildly reduced ejection fraction (HFmrEF). Limited data regarding the prognostic impact of the timing of onset of ADHF is available. Consecutive patients with HFmrEF and ADHF were retrospectively included at one institution from 2016 to 2022. Patients with primary ADHF were compared to patients with secondary ADHF with regard to the primary endpoint all-cause mortality at 30 months. Kaplan-Meier, uni- and multivariable Cox proportional regression analyses were applied for statistics. From a total of 484 patients hospitalized with HFmrEF and ADHF, 67.98% (n = 329) were admitted with primary ADHF. Patients with secondary ADHF had higher rates of concomitant acute myocardial infarction, alongside with a higher extend of coronary artery disease. The risk of all-cause mortality at 30 months was not affected by the timing of ADHF (hazard ratio (HR) = 0.853; 95% confidence interval (CI) 0.653-1.115; p = 0.246). However, patients with primary ADHF were associated with a higher risk of HF-related rehospitalization at 30 months (HR = 2.513; 95% CI 1.555-4.065; p = 0.001), which was still evident after multivariable adjustment (HR = 2.347; 95% CI 1.418-3.883; p = 0.001). The timing of onset of ADHF was not associated with long-term mortality in HFmrEF, however primary ADHF was associated with a higher risk of HF-related rehospitalization.</p>","PeriodicalId":12940,"journal":{"name":"Heart and Vessels","volume":" ","pages":"592-603"},"PeriodicalIF":1.5000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12165966/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Heart and Vessels","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00380-024-02505-3","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/22 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
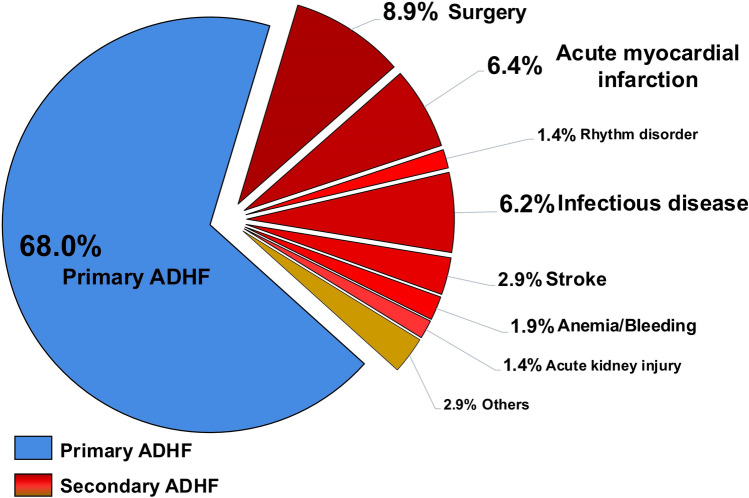
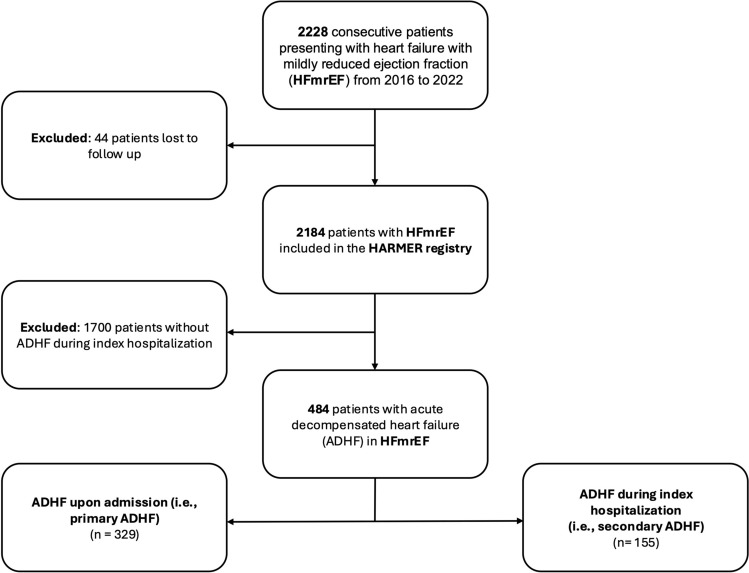
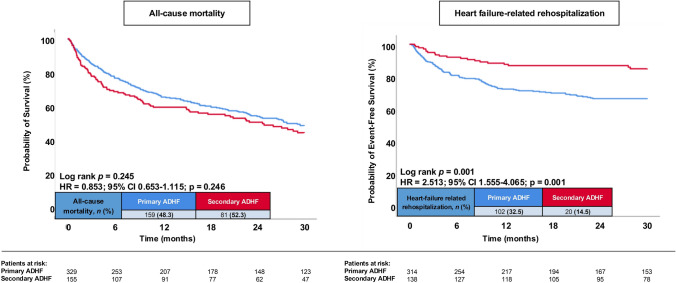
This study investigates the prognosis of acute decompensated heart failure (ADHF) on admission (i.e., primary ADHF) as compared to ADHF onset during course of hospitalization (i.e., secondary ADHF) in patients hospitalized with heart failure with mildly reduced ejection fraction (HFmrEF). Limited data regarding the prognostic impact of the timing of onset of ADHF is available. Consecutive patients with HFmrEF and ADHF were retrospectively included at one institution from 2016 to 2022. Patients with primary ADHF were compared to patients with secondary ADHF with regard to the primary endpoint all-cause mortality at 30 months. Kaplan-Meier, uni- and multivariable Cox proportional regression analyses were applied for statistics. From a total of 484 patients hospitalized with HFmrEF and ADHF, 67.98% (n = 329) were admitted with primary ADHF. Patients with secondary ADHF had higher rates of concomitant acute myocardial infarction, alongside with a higher extend of coronary artery disease. The risk of all-cause mortality at 30 months was not affected by the timing of ADHF (hazard ratio (HR) = 0.853; 95% confidence interval (CI) 0.653-1.115; p = 0.246). However, patients with primary ADHF were associated with a higher risk of HF-related rehospitalization at 30 months (HR = 2.513; 95% CI 1.555-4.065; p = 0.001), which was still evident after multivariable adjustment (HR = 2.347; 95% CI 1.418-3.883; p = 0.001). The timing of onset of ADHF was not associated with long-term mortality in HFmrEF, however primary ADHF was associated with a higher risk of HF-related rehospitalization.
期刊介绍:
Heart and Vessels is an English-language journal that provides a forum of original ideas, excellent methods, and fascinating techniques on cardiovascular disease fields. All papers submitted for publication are evaluated only with regard to scientific quality and relevance to the heart and vessels. Contributions from those engaged in practical medicine, as well as from those involved in basic research, are welcomed.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
