Adjunctive Intermittent Theta-Burst Stimulation for Schizophrenia: A Systematic Review and Meta-analysis of Randomized Double-Blind Controlled Studies.
{"title":"Adjunctive Intermittent Theta-Burst Stimulation for Schizophrenia: A Systematic Review and Meta-analysis of Randomized Double-Blind Controlled Studies.","authors":"Kai-Si Wen, Xin-Hu Yang, Nan Zhang, Si-Yuan Lin, Xing-Bing Huang, Todd Jackson, Yu-Tao Xiang, Wei Zheng","doi":"10.5152/alphapsychiatry.2024.241799","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>In order to determine whether intermittent theta-burst stimulation (iTBS) is a viable adjunct treatment for schizophrenia, a meta-analysis of double-blind, randomized clinical trials (RCTs) was performed.</p><p><strong>Methods: </strong>Four independent researchers extracted and synthesized data from RCTs on adjunctive iTBS for patients suffering from schizophrenia. RevMan 5.3 software was used to calculate risk ratios (RRs) and standardized mean differences (SMDs) along with their 95% confidence intervals (CIs).</p><p><strong>Results: </strong>Fifteen RCTs involving 671 patients with schizophrenia were included. Adjunctive iTBS was significantly superior to sham interventions for improvement in overall psychopathology (SMD = -0.75, 95% CI: -1.10, -0.41, <i>I</i> <sup>2</sup> = 64%, <i>P</i> < .0001), negative symptoms (SMD = -0.76, 95% CI: -1.18, -0.35, <i>I</i> <sup>2</sup> = 78%, <i>P</i> = .0003), and general psychopathology (SMD = -0.51, 95% CI: -0.88, -0.14, <i>I</i> <sup>2</sup> = 71%, <i>P</i> = .007), though no significant group difference was found regarding positive symptoms. Adjunctive iTBS also demonstrated superiority over control treatments in improving cognitive functions as measured by the Spatial Span Test (SMD = 0.83, 95% CI: 0.16, 1.49, <i>I</i> <sup>2</sup> = 73%, <i>P</i> = .02) and Montreal Cognitive Assessment (SMD = 0.49, 95% CI: 0.11, 0.88, <i>I</i> <sup>2</sup> = 0%, <i>P</i> = .01). Discontinuation rates (RR = 0.92, 95% CI: 0.57, 1.50, <i>I</i> <sup>2</sup> = 0%, <i>P</i> = .75) and adverse events were comparable between groups.</p><p><strong>Conclusion: </strong>The use of iTBS in patients with schizophrenia appears to be effective in improving psychiatric symptoms and cognitive function. To substantiate these preliminary findings, future research involving larger participant cohorts is warranted.</p>","PeriodicalId":72151,"journal":{"name":"Alpha psychiatry","volume":"25 6","pages":"676-684"},"PeriodicalIF":3.5000,"publicationDate":"2024-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11744375/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Alpha psychiatry","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5152/alphapsychiatry.2024.241799","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"PSYCHIATRY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: In order to determine whether intermittent theta-burst stimulation (iTBS) is a viable adjunct treatment for schizophrenia, a meta-analysis of double-blind, randomized clinical trials (RCTs) was performed.
Methods: Four independent researchers extracted and synthesized data from RCTs on adjunctive iTBS for patients suffering from schizophrenia. RevMan 5.3 software was used to calculate risk ratios (RRs) and standardized mean differences (SMDs) along with their 95% confidence intervals (CIs).
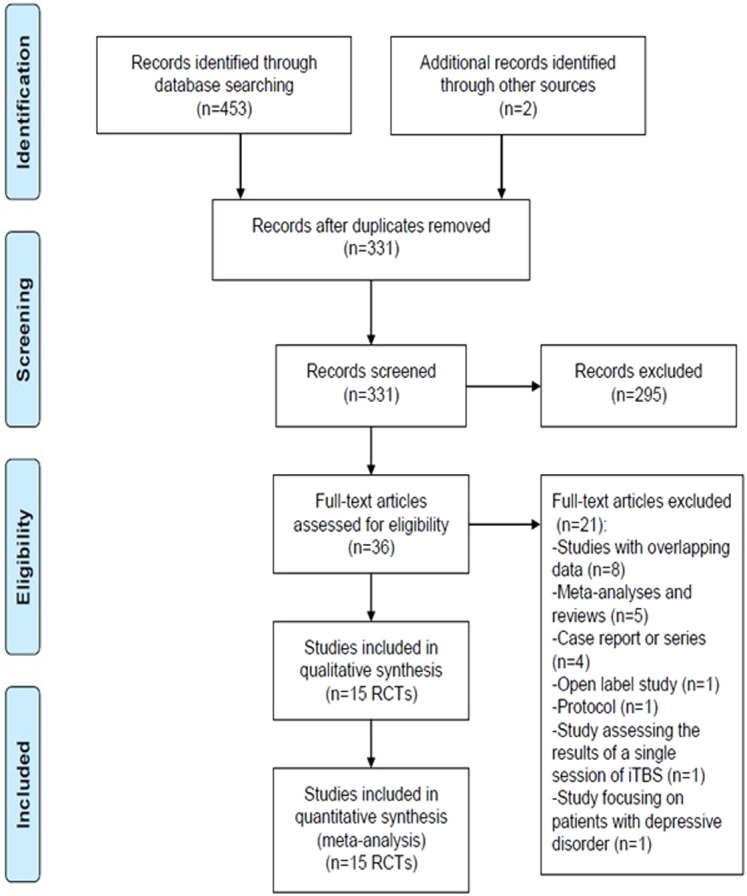
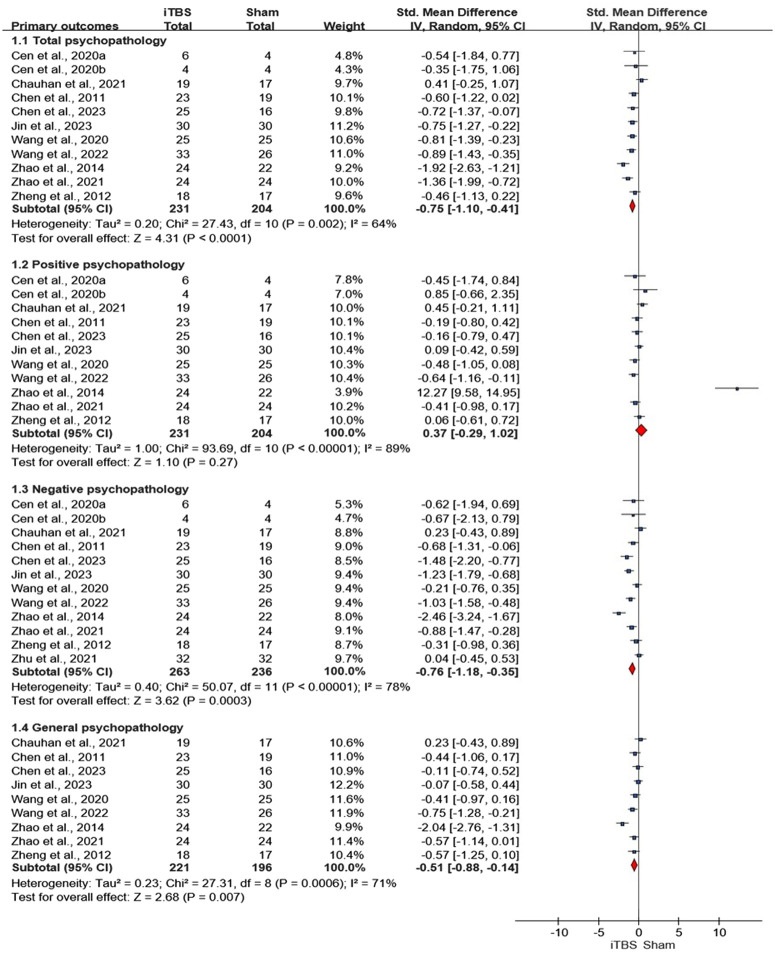
Results: Fifteen RCTs involving 671 patients with schizophrenia were included. Adjunctive iTBS was significantly superior to sham interventions for improvement in overall psychopathology (SMD = -0.75, 95% CI: -1.10, -0.41, I2 = 64%, P < .0001), negative symptoms (SMD = -0.76, 95% CI: -1.18, -0.35, I2 = 78%, P = .0003), and general psychopathology (SMD = -0.51, 95% CI: -0.88, -0.14, I2 = 71%, P = .007), though no significant group difference was found regarding positive symptoms. Adjunctive iTBS also demonstrated superiority over control treatments in improving cognitive functions as measured by the Spatial Span Test (SMD = 0.83, 95% CI: 0.16, 1.49, I2 = 73%, P = .02) and Montreal Cognitive Assessment (SMD = 0.49, 95% CI: 0.11, 0.88, I2 = 0%, P = .01). Discontinuation rates (RR = 0.92, 95% CI: 0.57, 1.50, I2 = 0%, P = .75) and adverse events were comparable between groups.
Conclusion: The use of iTBS in patients with schizophrenia appears to be effective in improving psychiatric symptoms and cognitive function. To substantiate these preliminary findings, future research involving larger participant cohorts is warranted.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
