Brennan Diedrich, Justin Roper, Benjamin Hopkins, Sibo Tian, Shadab Momin, Eduard Schreibmann, Aparna H. Kesarwala, Kirk Luca
{"title":"Integrating knowledge-based planning and noncoplanar oblique VMAT arcs: A study of dose to the heart and immune cells in thoracic radiotherapy","authors":"Brennan Diedrich, Justin Roper, Benjamin Hopkins, Sibo Tian, Shadab Momin, Eduard Schreibmann, Aparna H. Kesarwala, Kirk Luca","doi":"10.1016/j.tipsro.2025.100301","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><div>Recent patient studies have linked higher immune cell doses with worse quality of life and survival. For thoracic radiotherapy, heart dose is a major contributor to the effective dose to immune cells (EDIC).</div></div><div><h3>Purpose</h3><div>This study investigates heart and immune cell doses for plans optimized using a cardiac-sparing knowledge-based planning (KBP) model and the impact of carefully crafted beam geometry.</div></div><div><h3>Methods</h3><div>Sixteen stage III NSCLC patients previously treated to 60 Gy in 30 fractions using coplanar VMAT arcs were replanned using a cardiac-sparing KBP model with either the clinical field arrangement or noncoplanar oblique arcs that prioritize heart sparing. The cardiac-sparing KBP model consisted of fifteen substructures, all of which were used during optimization. All plans were normalized to 95% PTV coverage at 60 Gy. Statistical significance was assessed for EDIC (Jin Model), along with mean doses to the heart, lungs, body, and both the mean dose and D0.03 cc values for cardiac substructures, using the Wilcoxon signed-rank test.</div></div><div><h3>Results</h3><div>Compared to the clinically treated plans with the same beam geometry, cardiac-sparing KBP reduced mean heart dose from 8.50 Gy to 4.09 Gy and EDIC from 4.27 Gy to 3.81 Gy (p < 0.001). For the novel arcs, the mean heart dose was reduced to 3.70 Gy, significantly lower than KBP with clinical beam geometry (p = 0.001). EDIC, however, was equivalent. No statistically meaningful differences were observed for the remaining organs at risk, and all plans met institutional planning goals.</div></div><div><h3>Conclusion</h3><div>Cardiac-sparing RapidPlan is a valuable tool for reducing heart dose and lowering EDIC in NSCLC patients. Additional heart sparing is possible by strategically crafting noncoplanar oblique beams to minimize heart dose.</div></div>","PeriodicalId":36328,"journal":{"name":"Technical Innovations and Patient Support in Radiation Oncology","volume":"33 ","pages":"Article 100301"},"PeriodicalIF":2.8000,"publicationDate":"2025-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11780144/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Technical Innovations and Patient Support in Radiation Oncology","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2405632425000022","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/5 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"Nursing","Score":null,"Total":0}
引用次数: 0
Abstract
Background
Recent patient studies have linked higher immune cell doses with worse quality of life and survival. For thoracic radiotherapy, heart dose is a major contributor to the effective dose to immune cells (EDIC).
Purpose
This study investigates heart and immune cell doses for plans optimized using a cardiac-sparing knowledge-based planning (KBP) model and the impact of carefully crafted beam geometry.
Methods
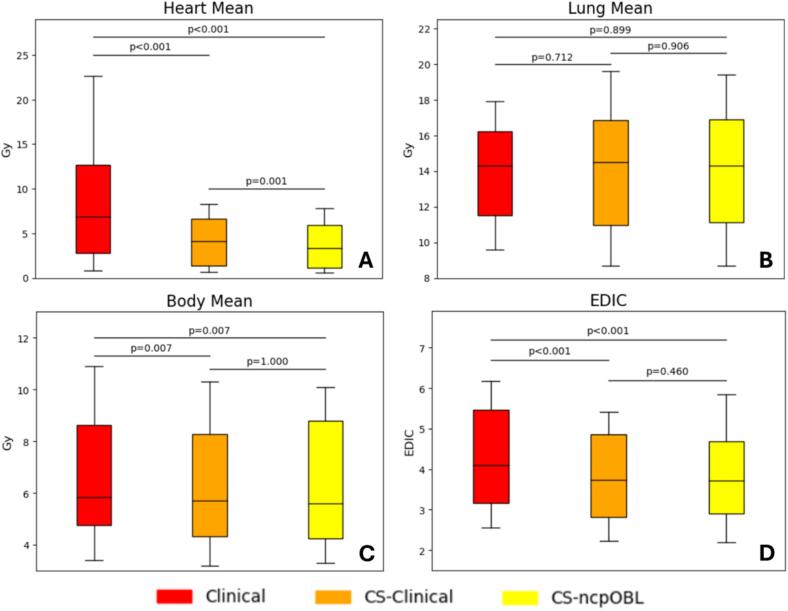
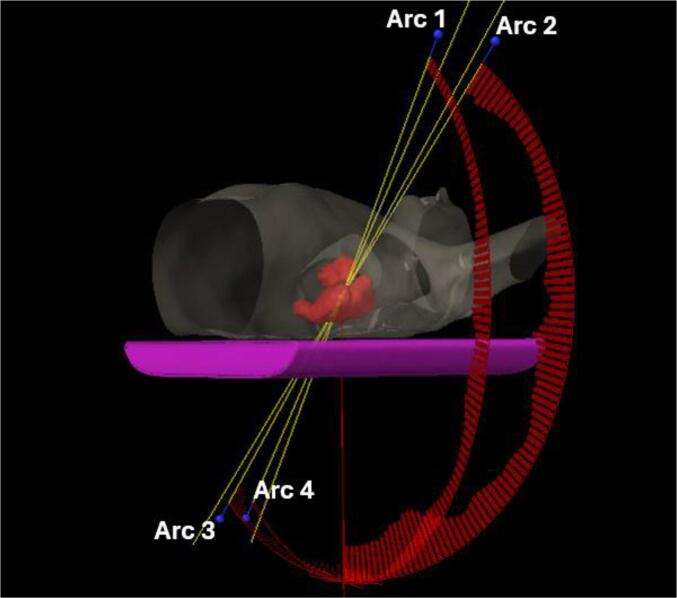
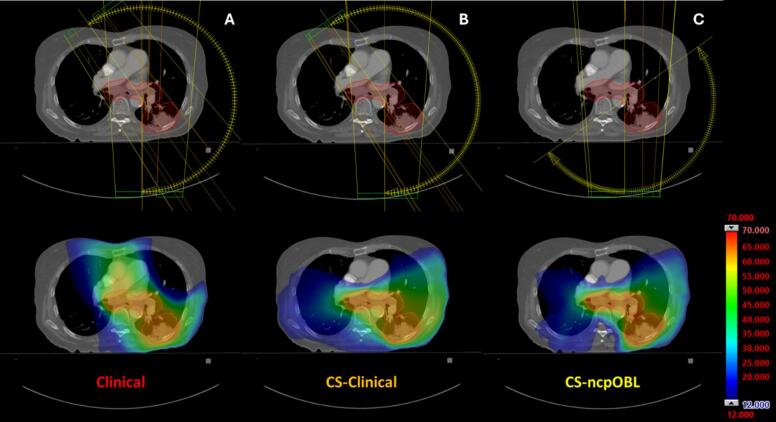
Sixteen stage III NSCLC patients previously treated to 60 Gy in 30 fractions using coplanar VMAT arcs were replanned using a cardiac-sparing KBP model with either the clinical field arrangement or noncoplanar oblique arcs that prioritize heart sparing. The cardiac-sparing KBP model consisted of fifteen substructures, all of which were used during optimization. All plans were normalized to 95% PTV coverage at 60 Gy. Statistical significance was assessed for EDIC (Jin Model), along with mean doses to the heart, lungs, body, and both the mean dose and D0.03 cc values for cardiac substructures, using the Wilcoxon signed-rank test.
Results
Compared to the clinically treated plans with the same beam geometry, cardiac-sparing KBP reduced mean heart dose from 8.50 Gy to 4.09 Gy and EDIC from 4.27 Gy to 3.81 Gy (p < 0.001). For the novel arcs, the mean heart dose was reduced to 3.70 Gy, significantly lower than KBP with clinical beam geometry (p = 0.001). EDIC, however, was equivalent. No statistically meaningful differences were observed for the remaining organs at risk, and all plans met institutional planning goals.
Conclusion
Cardiac-sparing RapidPlan is a valuable tool for reducing heart dose and lowering EDIC in NSCLC patients. Additional heart sparing is possible by strategically crafting noncoplanar oblique beams to minimize heart dose.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
