{"title":"Lobectomy Increases Postoperative Pulmonary Artery Enlargement to a Greater Extent than Segmentectomy.","authors":"Megumi Nishikubo, Yugo Tanaka, Shinya Tane, Daisuke Hokka, Yoshimasa Maniwa","doi":"10.5761/atcs.oa.24-00083","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>The underlying mechanism why segmentectomy has demonstrated the non-inferiority to lobectomy in several randomized trials remains unclear. Computed tomography (CT)-measured pulmonary artery (PA) enlargement reflects PA pressure and predicts the prognosis of certain respiratory diseases. We compared the preoperative and postoperative PA diameter to the ascending aorta diameter (PA/A) ratio, investigating its impact on right ventricular function in lung resection.</p><p><strong>Methods: </strong>This retrospective study was conducted in patients with lower-lobe lung tumors who underwent anatomical lung resection between 2017 and 2022. The PA diameter at the bifurcation and the ascending aorta diameter at the same CT image slice were measured preoperatively and postoperatively. We calculated the enlargement of PA/A ratio (PA/A change) and compared lobectomy and segmentectomy.</p><p><strong>Results: </strong>This analysis included 279 patients (235 with lobectomy and 44 with segmentectomy). The PA/A change was significantly greater in patients with lobectomy than segmentectomy (104% vs. 102%, P = 0.02). In the multivariable analysis, airflow obstruction (yes, P = 0.04) and the type of surgery (segmentectomy, P = 0.04) were independent prognostic factors for PA/A change.</p><p><strong>Conclusions: </strong>The PA/A change was greater in lobectomy than in segmentectomy. This change could reflect a burden on right ventricular function after lobectomy.</p>","PeriodicalId":93877,"journal":{"name":"Annals of thoracic and cardiovascular surgery : official journal of the Association of Thoracic and Cardiovascular Surgeons of Asia","volume":"31 1","pages":""},"PeriodicalIF":1.3000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11781968/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of thoracic and cardiovascular surgery : official journal of the Association of Thoracic and Cardiovascular Surgeons of Asia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5761/atcs.oa.24-00083","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: The underlying mechanism why segmentectomy has demonstrated the non-inferiority to lobectomy in several randomized trials remains unclear. Computed tomography (CT)-measured pulmonary artery (PA) enlargement reflects PA pressure and predicts the prognosis of certain respiratory diseases. We compared the preoperative and postoperative PA diameter to the ascending aorta diameter (PA/A) ratio, investigating its impact on right ventricular function in lung resection.
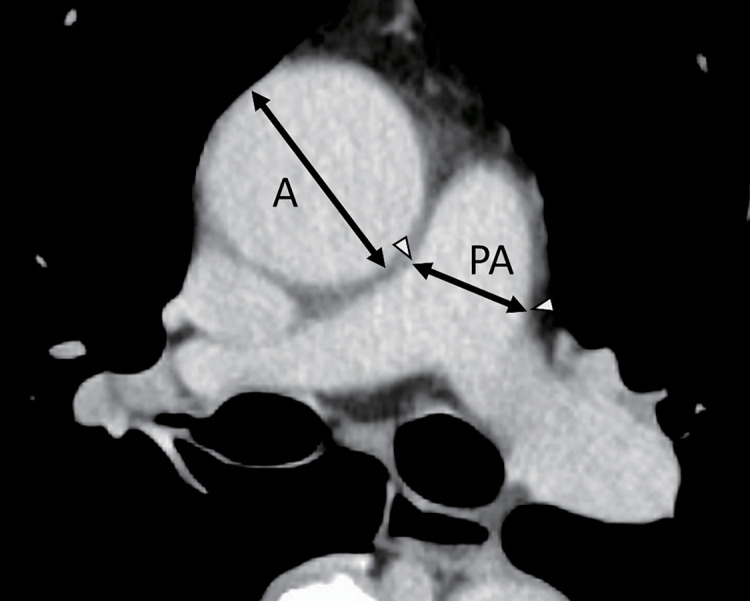
Methods: This retrospective study was conducted in patients with lower-lobe lung tumors who underwent anatomical lung resection between 2017 and 2022. The PA diameter at the bifurcation and the ascending aorta diameter at the same CT image slice were measured preoperatively and postoperatively. We calculated the enlargement of PA/A ratio (PA/A change) and compared lobectomy and segmentectomy.
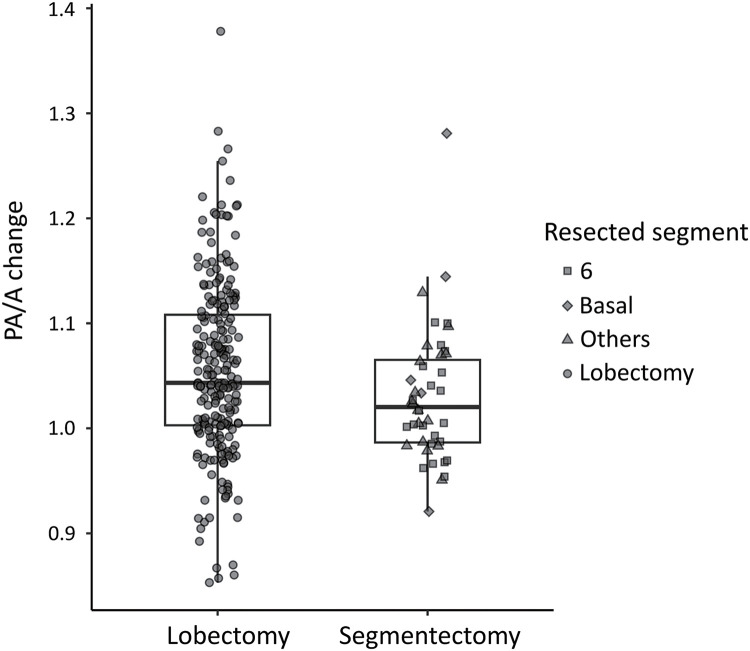
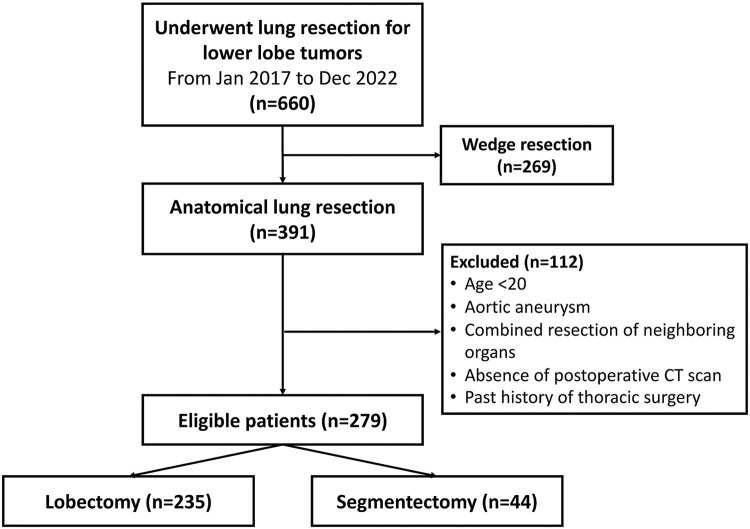
Results: This analysis included 279 patients (235 with lobectomy and 44 with segmentectomy). The PA/A change was significantly greater in patients with lobectomy than segmentectomy (104% vs. 102%, P = 0.02). In the multivariable analysis, airflow obstruction (yes, P = 0.04) and the type of surgery (segmentectomy, P = 0.04) were independent prognostic factors for PA/A change.
Conclusions: The PA/A change was greater in lobectomy than in segmentectomy. This change could reflect a burden on right ventricular function after lobectomy.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
