Use of intravenous immunoglobulin for the treatment of severe COVID-19 in the Chris Hani Baragwanath Academic Hospital intensive care unit, Johannesburg, South Africa.
{"title":"Use of intravenous immunoglobulin for the treatment of severe COVID-19 in the Chris Hani Baragwanath Academic Hospital intensive care unit, Johannesburg, South Africa.","authors":"G Mensky, A van Blydenstein, J Damelin, S Omar","doi":"10.7196/SAJCC.2024.v40i3.1897","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>COVID-19 infection has a variable clinical presentation, with a small subgroup of patients developing severe disease, requiring intensive care with mechanical ventilation, with an increased mortality rate. South Africa (SA) has experienced multiple waves of this pandemic, spanning the pre-vaccine and vaccine periods. The method and initiation of treatment is a debated topic, changing according to evolving research and the literature. The present study investigated the use of high-dose intravenous immunoglobulin (IVIg) as a salvage therapy after initial medical treatment failure.</p><p><strong>Objectives: </strong>To compare disease progression among critically ill COVID-19 pneumonia patients receiving IVIg therapy with that in patients receiving standard of care (SoC), in respect of inflammation, organ dysfunction and oxygenation.</p><p><strong>Methods: </strong>This was a single-centre, retrospective study of patients admitted to the intensive care unit (ICU) at Chris Hani Baragwanath Academic Hospital, Johannesburg, SA, during the pre-vaccine COVID-19 pandemic. Demographics, inflammatory markers (C-reactive protein (CRP)), organ function (Sequential Organ Failure Assessment (SOFA) score), oxygenation (ratio of partial pressure of oxygen in arterial blood to fraction of inspiratory oxygen (P/F ratio)), overall mortality and complications (nosocomial infections and thromboembolism) were recorded and compared.</p><p><strong>Results: </strong>We included 113 eligible patients in the study. The IVIg cohort had a significantly lower initial P/F ratio than the SoC cohort (p=0.01), but the change in P/F ratio was similar (p=0.54). Initial CRP and changes in CRP were similar in the two groups (p=0.38 and p=0.75, respectively), as were initial SOFA score and changes in SOFA score (p=0.18 and p=0.08, respectively) and vasopressor dose on day 0 and day 5 (p=0.97 and p=0.93, respectively). Duration of mechanical ventilation did not differ significantly between the IVIg group and the SoC group (p=0.13). There were no significant differences in measured complications between the two groups. On univariate analysis, the relative risk of death was 1.6 times higher (95% confidence interval (CI) 1.1 - 2.3) in the IVIg group; however, a logistical regression model demonstrated that only a higher P/F ratio (odds ratio (OR) 0.991; 95% CI 0.983 - 0.997) and higher mean airway pressure (OR 1.283; 95% CI 1.026 - 1.604) were significantly associated with ICU mortality.</p><p><strong>Conclusion: </strong>Use of IVIg in our study was directed at an older population, with significantly worse oxygenation. We found no evidence of adverse effects of immunoglobulin therapy; however, we found no benefit either. Only the P/F ratio and mean airway pressure independently predicted ICU mortality.</p><p><strong>Contribution of the study: </strong>During the COVID-19 pandemic, treatment protocols changed in response to the evolving literature. Hospitals were faced with choosing a treatment modality that they believed at the time had benefit. Chris Hani Baragwanath Hospital in Johannesburg, South Africa (SA), incorporated IVIg into its treatment protocols for patients with severe COVID pneumonia requiring ICU admission. This study retrospectively analysed the use of IVIg therapy in the hope of creating a more robust understanding of its safety and efficacy as a treatment option for SA patients in the future.</p>","PeriodicalId":75194,"journal":{"name":"The Southern African journal of critical care : the official journal of the Critical Care Society","volume":"40 3","pages":"e1897"},"PeriodicalIF":0.0000,"publicationDate":"2024-11-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11792588/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"The Southern African journal of critical care : the official journal of the Critical Care Society","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.7196/SAJCC.2024.v40i3.1897","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: COVID-19 infection has a variable clinical presentation, with a small subgroup of patients developing severe disease, requiring intensive care with mechanical ventilation, with an increased mortality rate. South Africa (SA) has experienced multiple waves of this pandemic, spanning the pre-vaccine and vaccine periods. The method and initiation of treatment is a debated topic, changing according to evolving research and the literature. The present study investigated the use of high-dose intravenous immunoglobulin (IVIg) as a salvage therapy after initial medical treatment failure.
Objectives: To compare disease progression among critically ill COVID-19 pneumonia patients receiving IVIg therapy with that in patients receiving standard of care (SoC), in respect of inflammation, organ dysfunction and oxygenation.
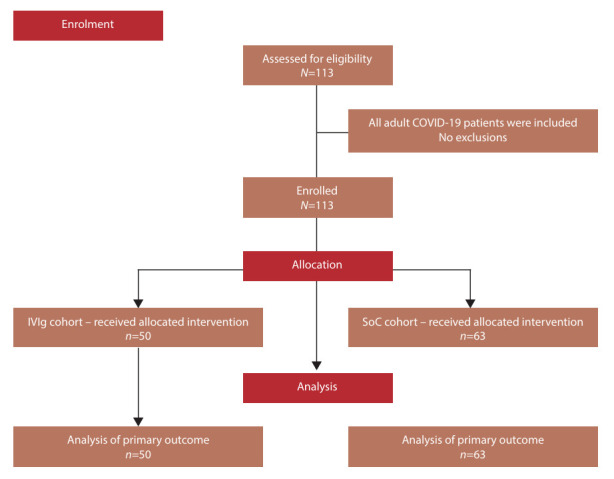
Methods: This was a single-centre, retrospective study of patients admitted to the intensive care unit (ICU) at Chris Hani Baragwanath Academic Hospital, Johannesburg, SA, during the pre-vaccine COVID-19 pandemic. Demographics, inflammatory markers (C-reactive protein (CRP)), organ function (Sequential Organ Failure Assessment (SOFA) score), oxygenation (ratio of partial pressure of oxygen in arterial blood to fraction of inspiratory oxygen (P/F ratio)), overall mortality and complications (nosocomial infections and thromboembolism) were recorded and compared.
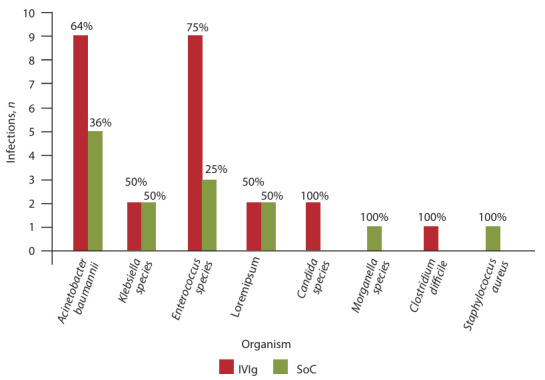
Results: We included 113 eligible patients in the study. The IVIg cohort had a significantly lower initial P/F ratio than the SoC cohort (p=0.01), but the change in P/F ratio was similar (p=0.54). Initial CRP and changes in CRP were similar in the two groups (p=0.38 and p=0.75, respectively), as were initial SOFA score and changes in SOFA score (p=0.18 and p=0.08, respectively) and vasopressor dose on day 0 and day 5 (p=0.97 and p=0.93, respectively). Duration of mechanical ventilation did not differ significantly between the IVIg group and the SoC group (p=0.13). There were no significant differences in measured complications between the two groups. On univariate analysis, the relative risk of death was 1.6 times higher (95% confidence interval (CI) 1.1 - 2.3) in the IVIg group; however, a logistical regression model demonstrated that only a higher P/F ratio (odds ratio (OR) 0.991; 95% CI 0.983 - 0.997) and higher mean airway pressure (OR 1.283; 95% CI 1.026 - 1.604) were significantly associated with ICU mortality.
Conclusion: Use of IVIg in our study was directed at an older population, with significantly worse oxygenation. We found no evidence of adverse effects of immunoglobulin therapy; however, we found no benefit either. Only the P/F ratio and mean airway pressure independently predicted ICU mortality.
Contribution of the study: During the COVID-19 pandemic, treatment protocols changed in response to the evolving literature. Hospitals were faced with choosing a treatment modality that they believed at the time had benefit. Chris Hani Baragwanath Hospital in Johannesburg, South Africa (SA), incorporated IVIg into its treatment protocols for patients with severe COVID pneumonia requiring ICU admission. This study retrospectively analysed the use of IVIg therapy in the hope of creating a more robust understanding of its safety and efficacy as a treatment option for SA patients in the future.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
