L. S. Johnson, P. Zadrozniak, G. Jasina, A. Grotek-Cuprjak, J. G. Andrade, E. Svennberg, S. Z. Diederichsen, W. F. McIntyre, S. Stavrakis, J. Benezet-Mazuecos, P. Krisai, Z. Iakobishvili, A. Laish-Farkash, S. Bhavnani, E. Ljungström, J. Bacevicius, N. L. van Vreeswijk, M. Rienstra, R. Spittler, J. A. Marx, A. Oraii, A. Miracle Blanco, A. Lozano, I. Mustafina, S. Zafeiropoulos, R. Bennett, J. Bisson, D. Linz, Y. Kogan, E. Glazer, G. Marincheva, M. Rahkovich, E. Shaked, M. H. Ruwald, K. Haugan, J. Węcławski, G. Radoslovich, S. Jamal, A. Brandes, P. T. Matusik, M. Manninger, P. B. Meyre, S. Blum, A. Persson, A. Måneheim, P. Hammarlund, A. Fedorowski, T. Wodaje, C. Lewinter, V. Juknevicius, R. Jakaite, C. Shen, T. Glotzer, P. Platonov, G. Engström, A. P. Benz, J. S. Healey
{"title":"Artificial intelligence for direct-to-physician reporting of ambulatory electrocardiography","authors":"L. S. Johnson, P. Zadrozniak, G. Jasina, A. Grotek-Cuprjak, J. G. Andrade, E. Svennberg, S. Z. Diederichsen, W. F. McIntyre, S. Stavrakis, J. Benezet-Mazuecos, P. Krisai, Z. Iakobishvili, A. Laish-Farkash, S. Bhavnani, E. Ljungström, J. Bacevicius, N. L. van Vreeswijk, M. Rienstra, R. Spittler, J. A. Marx, A. Oraii, A. Miracle Blanco, A. Lozano, I. Mustafina, S. Zafeiropoulos, R. Bennett, J. Bisson, D. Linz, Y. Kogan, E. Glazer, G. Marincheva, M. Rahkovich, E. Shaked, M. H. Ruwald, K. Haugan, J. Węcławski, G. Radoslovich, S. Jamal, A. Brandes, P. T. Matusik, M. Manninger, P. B. Meyre, S. Blum, A. Persson, A. Måneheim, P. Hammarlund, A. Fedorowski, T. Wodaje, C. Lewinter, V. Juknevicius, R. Jakaite, C. Shen, T. Glotzer, P. Platonov, G. Engström, A. P. Benz, J. S. Healey","doi":"10.1038/s41591-025-03516-x","DOIUrl":null,"url":null,"abstract":"Developments in ambulatory electrocardiogram (ECG) technology have led to vast amounts of ECG data that currently need to be interpreted by human technicians. Here we tested an artificial intelligence (AI) algorithm for direct-to-physician reporting of ambulatory ECGs. Beat-by-beat annotation of 14,606 individual ambulatory ECG recordings (mean duration = 14 ± 10 days) was performed by certified ECG technicians (n = 167) and an ensemble AI model, called DeepRhythmAI. To compare the performance of the AI model and the technicians, a random sample of 5,235 rhythm events identified by the AI model or by technicians, of which 2,236 events were identified as critical arrhythmias, was selected for annotation by one of 17 cardiologist consensus panels. The mean sensitivity of the AI model for the identification of critical arrhythmias was 98.6% (95% confidence interval (CI) = 97.7–99.4), as compared to 80.3% (95% CI = 77.3–83.3%) for the technicians. False-negative findings were observed in 3.2/1,000 patients for the AI model versus 44.3/1,000 patients for the technicians. Accordingly, the relative risk of a missed diagnosis was 14.1 (95% CI = 10.4–19.0) times higher for the technicians. However, a higher false-positive event rate was observed for the AI model (12 (interquartile range (IQR) = 6–74)/1,000 patient days) as compared to the technicians (5 (IQR = 2–153)/1,000 patient days). We conclude that the DeepRhythmAI model has excellent negative predictive value for critical arrhythmias, substantially reducing false-negative findings, but at a modest cost of increased false-positive findings. AI-only analysis to facilitate direct-to-physician reporting could potentially reduce costs and improve access to care and outcomes in patients who need ambulatory ECG monitoring. In a large-scale analysis of ambulatory electrocardiographic recordings, a deep learning algorithm had a substantially higher sensitivity for the detection of critical arrhythmias as compared to technicians, opening a path toward artificial intelligence-assisted direct-to-physician reporting of ambulatory electrocardiography results.","PeriodicalId":19037,"journal":{"name":"Nature Medicine","volume":"31 3","pages":"925-931"},"PeriodicalIF":50.0000,"publicationDate":"2025-02-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.nature.com/articles/s41591-025-03516-x.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Nature Medicine","FirstCategoryId":"3","ListUrlMain":"https://www.nature.com/articles/s41591-025-03516-x","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"BIOCHEMISTRY & MOLECULAR BIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
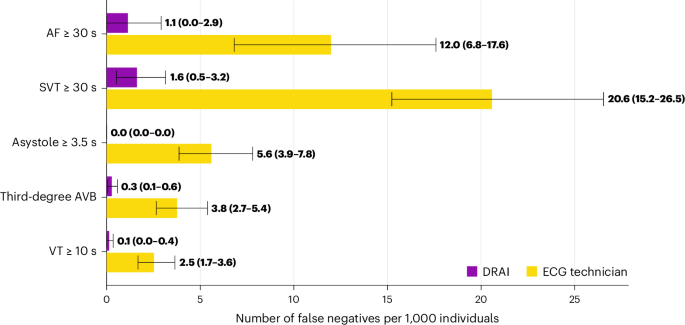
Developments in ambulatory electrocardiogram (ECG) technology have led to vast amounts of ECG data that currently need to be interpreted by human technicians. Here we tested an artificial intelligence (AI) algorithm for direct-to-physician reporting of ambulatory ECGs. Beat-by-beat annotation of 14,606 individual ambulatory ECG recordings (mean duration = 14 ± 10 days) was performed by certified ECG technicians (n = 167) and an ensemble AI model, called DeepRhythmAI. To compare the performance of the AI model and the technicians, a random sample of 5,235 rhythm events identified by the AI model or by technicians, of which 2,236 events were identified as critical arrhythmias, was selected for annotation by one of 17 cardiologist consensus panels. The mean sensitivity of the AI model for the identification of critical arrhythmias was 98.6% (95% confidence interval (CI) = 97.7–99.4), as compared to 80.3% (95% CI = 77.3–83.3%) for the technicians. False-negative findings were observed in 3.2/1,000 patients for the AI model versus 44.3/1,000 patients for the technicians. Accordingly, the relative risk of a missed diagnosis was 14.1 (95% CI = 10.4–19.0) times higher for the technicians. However, a higher false-positive event rate was observed for the AI model (12 (interquartile range (IQR) = 6–74)/1,000 patient days) as compared to the technicians (5 (IQR = 2–153)/1,000 patient days). We conclude that the DeepRhythmAI model has excellent negative predictive value for critical arrhythmias, substantially reducing false-negative findings, but at a modest cost of increased false-positive findings. AI-only analysis to facilitate direct-to-physician reporting could potentially reduce costs and improve access to care and outcomes in patients who need ambulatory ECG monitoring. In a large-scale analysis of ambulatory electrocardiographic recordings, a deep learning algorithm had a substantially higher sensitivity for the detection of critical arrhythmias as compared to technicians, opening a path toward artificial intelligence-assisted direct-to-physician reporting of ambulatory electrocardiography results.
期刊介绍:
Nature Medicine is a monthly journal publishing original peer-reviewed research in all areas of medicine. The publication focuses on originality, timeliness, interdisciplinary interest, and the impact on improving human health. In addition to research articles, Nature Medicine also publishes commissioned content such as News, Reviews, and Perspectives. This content aims to provide context for the latest advances in translational and clinical research, reaching a wide audience of M.D. and Ph.D. readers. All editorial decisions for the journal are made by a team of full-time professional editors.
Nature Medicine consider all types of clinical research, including:
-Case-reports and small case series
-Clinical trials, whether phase 1, 2, 3 or 4
-Observational studies
-Meta-analyses
-Biomarker studies
-Public and global health studies
Nature Medicine is also committed to facilitating communication between translational and clinical researchers. As such, we consider “hybrid” studies with preclinical and translational findings reported alongside data from clinical studies.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
