{"title":"Medicare Advantage penetration and the financial distress of rural hospitals.","authors":"Guido Cataife, Siying Liu","doi":"10.1186/s13561-025-00599-7","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Medicare Advantage (MA) penetration rates have shown an increase in rural areas in the past decade, increasing the bargaining power of MA plans relative to rural hospitals. We study the effect that this increase has had in the revenue of rural hospitals through reductions in the number of inpatient days paid by the plans, which has been reported to be part of the financial bargaining between the two parties.</p><p><strong>Methods: </strong>We use 2014-2020 hospital level data from the American Hospital Association's annual survey and county-level MA penetration rates. We estimate the correlation between MA penetration rates and Medicare and non-Medicare inpatient days using multivariate regressions with hospital and year fixed effects. We use results for urban areas where competition among multiple MA sponsors reduces their individual bargaining power as a falsification test.</p><p><strong>Results: </strong>We find that a 10 percentage points increase in the county-level MA penetration rate is associated with a decrease of 0.87% inpatient days paid to rural hospitals, which unveils a new main factor affecting the fragile finances of rural hospitals. Consistent with our hypothesis, urban hospitals do not exhibit similar effects, underscoring the role of MA plans in rural areas.</p><p><strong>Conclusions: </strong>As MA plans increase their penetration in rural areas, their bargaining power increases relative to rural hospitals. MA plans use this increased bargaining power to reduce the number of paid inpatient days, which creates adverse financial conditions for rural hospitals. Policymakers can safeguard rural hospitals by modifying the fee-for-service prices received by rural hospitals or strengthening the network adequacy criteria of MA plans for rural areas.</p>","PeriodicalId":46936,"journal":{"name":"Health Economics Review","volume":"15 1","pages":"9"},"PeriodicalIF":3.3000,"publicationDate":"2025-02-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11817615/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Health Economics Review","FirstCategoryId":"96","ListUrlMain":"https://doi.org/10.1186/s13561-025-00599-7","RegionNum":3,"RegionCategory":"经济学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ECONOMICS","Score":null,"Total":0}
引用次数: 0
Abstract
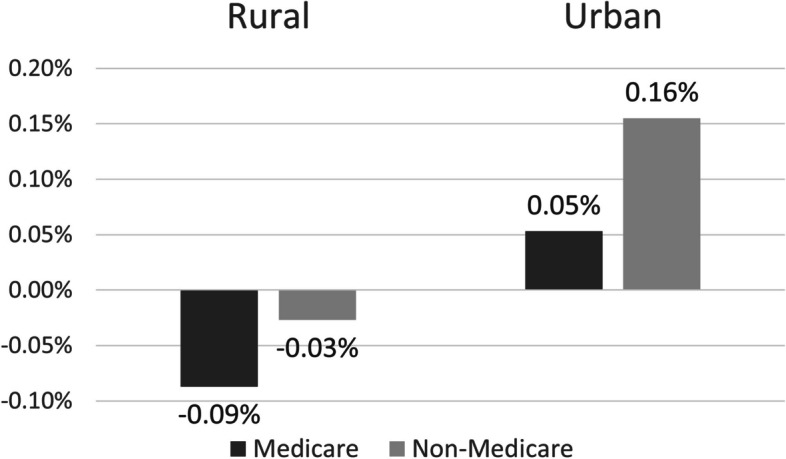
Background: Medicare Advantage (MA) penetration rates have shown an increase in rural areas in the past decade, increasing the bargaining power of MA plans relative to rural hospitals. We study the effect that this increase has had in the revenue of rural hospitals through reductions in the number of inpatient days paid by the plans, which has been reported to be part of the financial bargaining between the two parties.
Methods: We use 2014-2020 hospital level data from the American Hospital Association's annual survey and county-level MA penetration rates. We estimate the correlation between MA penetration rates and Medicare and non-Medicare inpatient days using multivariate regressions with hospital and year fixed effects. We use results for urban areas where competition among multiple MA sponsors reduces their individual bargaining power as a falsification test.
Results: We find that a 10 percentage points increase in the county-level MA penetration rate is associated with a decrease of 0.87% inpatient days paid to rural hospitals, which unveils a new main factor affecting the fragile finances of rural hospitals. Consistent with our hypothesis, urban hospitals do not exhibit similar effects, underscoring the role of MA plans in rural areas.
Conclusions: As MA plans increase their penetration in rural areas, their bargaining power increases relative to rural hospitals. MA plans use this increased bargaining power to reduce the number of paid inpatient days, which creates adverse financial conditions for rural hospitals. Policymakers can safeguard rural hospitals by modifying the fee-for-service prices received by rural hospitals or strengthening the network adequacy criteria of MA plans for rural areas.
期刊介绍:
Health Economics Review is an international high-quality journal covering all fields of Health Economics. A broad range of theoretical contributions, empirical studies and analyses of health policy with a health economic focus will be considered for publication. Its scope includes macro- and microeconomics of health care financing, health insurance and reimbursement as well as health economic evaluation, health services research and health policy analysis. Further research topics are the individual and institutional aspects of health care management and the growing importance of health care in developing countries.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
