Wei Ru, Hongbo Liu, Juan Zhou, Qibo Hu, Weifeng Yang, Lizhe Hu, Guangjie Chen, Xiang Yan
{"title":"Diagnostic Accuracy of Uroflowmetry for Urethral Strictures in Pediatric Hypospadias: TIP versus Non-TIP Outcomes.","authors":"Wei Ru, Hongbo Liu, Juan Zhou, Qibo Hu, Weifeng Yang, Lizhe Hu, Guangjie Chen, Xiang Yan","doi":"10.1055/a-2536-4549","DOIUrl":null,"url":null,"abstract":"<p><p>This study aimed to evaluate the diagnostic accuracy of uroflowmetry in detecting pediatric urethral strictures following tubularized incised plate (TIP) and non-TIP urethroplasty.A retrospective cohort study was conducted on children who underwent primary hypospadias repairs from June 2016 to June 2023 at our institution. Patients were categorized into the TIP and the non-TIP groups. Urethral calibration and uroflowmetry were used to evaluate urethral patency following urethroplasty. Data on demographic characteristics, perioperative information, uroflowmetry results, urethral calibration outcomes, and postoperative complications were collected.The relationship between calibration and uroflowmetry and the diagnostic accuracy of uroflowmetry for urethral strictures were analyzed.A total of 62 cases were included, with 38 in the TIP group and 24 in the non-TIP group. Ten patients were diagnosed with urethral strictures. The maximum urinary flow rate (Q<sub>max</sub>) exhibited a higher area under the curve (AUC) than the average urinary flow rate (Q<sub>ave</sub>) in both the TIP and non-TIP groups. The Q<sub>max</sub> in the non-TIP group demonstrated a higher AUC than in the TIP group (non-TIP: AUC = 0.94, cutoff = 6.65 ml/s, sensitivity = 100%, specificity = 81.0%; TIP: AUC = 0.80, cutoff = 5.75 ml/s, sensitivity = 100%, specificity = 58.1%). A significant quadratic correlation was found between Q<sub>max</sub> and urethral calibration (non-TIP: <i>C</i> <sup>2</sup> = 14.72 * Q<sub>max</sub>, <i>R</i> <sup>2</sup> = 0.96; TIP: <i>C</i> <sup>2</sup> = 14.76 * Q<sub>max</sub>, <i>R</i> <sup>2</sup> = 0.88). The Q<sub>max</sub> nomogram interval ≤ -3 standard deviation was a significant predictor for non-TIP urethral strictures (kappa = 0.70).Uroflowmetry, particularly Q<sub>max</sub>, shows promise as a noninvasive screening tool for detecting urethral strictures after hypospadias repair. It has high diagnostic accuracy in non-TIP cases but limited utility in TIP cases.</p>","PeriodicalId":56316,"journal":{"name":"European Journal of Pediatric Surgery","volume":" ","pages":"309-315"},"PeriodicalIF":1.4000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12245517/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Journal of Pediatric Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1055/a-2536-4549","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/2/11 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
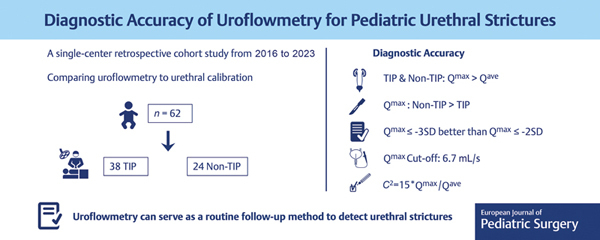
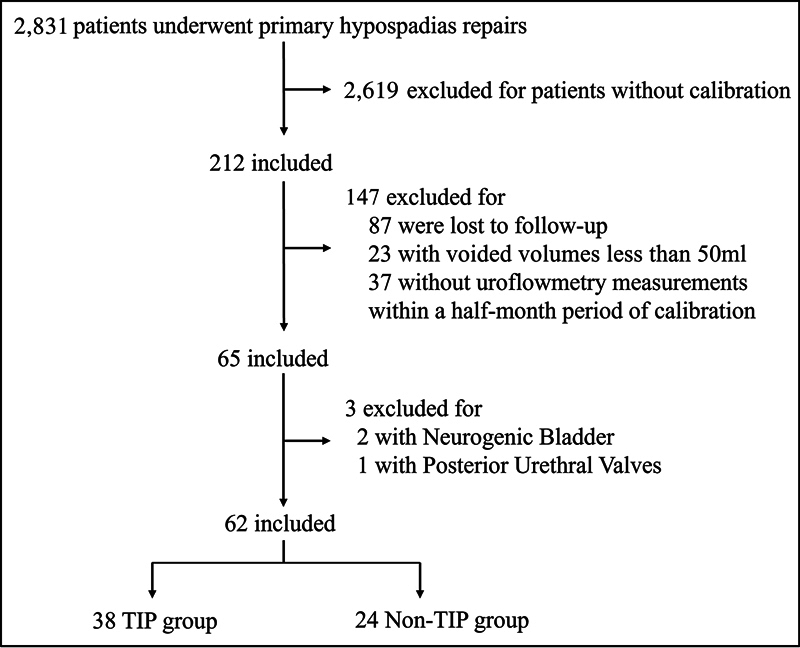
This study aimed to evaluate the diagnostic accuracy of uroflowmetry in detecting pediatric urethral strictures following tubularized incised plate (TIP) and non-TIP urethroplasty.A retrospective cohort study was conducted on children who underwent primary hypospadias repairs from June 2016 to June 2023 at our institution. Patients were categorized into the TIP and the non-TIP groups. Urethral calibration and uroflowmetry were used to evaluate urethral patency following urethroplasty. Data on demographic characteristics, perioperative information, uroflowmetry results, urethral calibration outcomes, and postoperative complications were collected.The relationship between calibration and uroflowmetry and the diagnostic accuracy of uroflowmetry for urethral strictures were analyzed.A total of 62 cases were included, with 38 in the TIP group and 24 in the non-TIP group. Ten patients were diagnosed with urethral strictures. The maximum urinary flow rate (Qmax) exhibited a higher area under the curve (AUC) than the average urinary flow rate (Qave) in both the TIP and non-TIP groups. The Qmax in the non-TIP group demonstrated a higher AUC than in the TIP group (non-TIP: AUC = 0.94, cutoff = 6.65 ml/s, sensitivity = 100%, specificity = 81.0%; TIP: AUC = 0.80, cutoff = 5.75 ml/s, sensitivity = 100%, specificity = 58.1%). A significant quadratic correlation was found between Qmax and urethral calibration (non-TIP: C2 = 14.72 * Qmax, R2 = 0.96; TIP: C2 = 14.76 * Qmax, R2 = 0.88). The Qmax nomogram interval ≤ -3 standard deviation was a significant predictor for non-TIP urethral strictures (kappa = 0.70).Uroflowmetry, particularly Qmax, shows promise as a noninvasive screening tool for detecting urethral strictures after hypospadias repair. It has high diagnostic accuracy in non-TIP cases but limited utility in TIP cases.
期刊介绍:
This broad-based international journal updates you on vital developments in pediatric surgery through original articles, abstracts of the literature, and meeting announcements.
You will find state-of-the-art information on:
abdominal and thoracic surgery
neurosurgery
urology
gynecology
oncology
orthopaedics
traumatology
anesthesiology
child pathology
embryology
morphology
Written by surgeons, physicians, anesthesiologists, radiologists, and others involved in the surgical care of neonates, infants, and children, the EJPS is an indispensable resource for all specialists.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
