Andrea Sauer, Klaus Stahl, Benjamin Seeliger, Pedro David Wendel-Garcia, Felix Lehmann, Julius J Schmidt, Bernhard M W Schmidt, Tobias Welte, Konrad Peukert, Lennart Wild, Christian Putensen, Sascha David, Christian Bode
{"title":"The effect of therapeutic plasma exchange on the inflammatory response in septic shock: a secondary analysis of the EXCHANGE-1 trial.","authors":"Andrea Sauer, Klaus Stahl, Benjamin Seeliger, Pedro David Wendel-Garcia, Felix Lehmann, Julius J Schmidt, Bernhard M W Schmidt, Tobias Welte, Konrad Peukert, Lennart Wild, Christian Putensen, Sascha David, Christian Bode","doi":"10.1186/s40635-025-00725-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Sepsis and septic shock, defined by a profound immune dysregulation, are among the leading causes of death in the intensive care unit (ICU). Despite advances in understanding the underlying pathophysiology, evidence for specific immunomodulatory treatment does not exist to date. Therapeutic plasma exchange (TPE) represents an adjunctive treatment approach to rebalance immune homeostasis. In the EXCHANGE-1 trial, we recently demonstrated a rapid hemodynamic improvement, possibly caused by the removal of harmful mediators and the replacement of protective plasma proteins. The aim of this secondary analysis is to further characterize the underlying immunomodulatory effects and to identify biomarkers that may predict treatment response.</p><p><strong>Methods: </strong>This secondary analysis included patients in early septic shock (< 24 h duration) and a norepinephrine (NE) dose of ≥ 0.4 μg/kg/min. Patients were randomized 1:1 to receive standard of care (SOC) or SOC + one single TPE and plasma samples were collected before and after TPE. Within-group and between group effects of circulating levels of acute-phase proteins [CRP and Pentraxin3 (PTX3)], inflammatory mediators (IL-4, IL-6, IL-8, IL-10, TNF-α, IL-2Rα/CD25) and damage-associated molecular pattern (DAMP) [cell-free DNA (cfDNA)] were analyzed via paired t test or Wilcoxon signed-rank test and a mixed-effects model. Multivariate mixed-effects modeling of NE and lactate reduction was performed to investigate if cfDNA could be associated with treatment response to TPE.</p><p><strong>Results: </strong>TPE led to a significant reduction in circulating acute-phase protein levels (CRP p = 0.00976, PTX3 p = 0.0001). Pro-inflammatory cytokines, such as circulating TNF-α-, IL-6- und IL-8-levels, were significantly reduced in both groups with no significant difference between treatment groups except for IL-2Rα/CD25 (p ≤ 0.0001). In a multivariate mixed-effects model, rising cfDNA levels over the first 6 h indicated refractoriness to SOC treatment regarding NE (p = 0.004) and lactate (p = 0.001), whereas those receiving TPE demonstrated sustained reductions in both parameters.</p><p><strong>Conclusions: </strong>In this secondary analysis of the EXCHANGE-1 trial adjunctive TPE is associated with the reduction of acute-phase proteins and IL-2Rα/CD25, however not with the reduction of pro-inflammatory cytokines. This phenomenon could contribute to the observed enhancement in hemodynamics among patients with septic shock. Furthermore, TPE may be particularly beneficial for patients with septic shock who exhibit rising levels of cfDNA.</p>","PeriodicalId":13750,"journal":{"name":"Intensive Care Medicine Experimental","volume":"13 1","pages":"18"},"PeriodicalIF":2.8000,"publicationDate":"2025-02-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11828778/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Intensive Care Medicine Experimental","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40635-025-00725-z","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Sepsis and septic shock, defined by a profound immune dysregulation, are among the leading causes of death in the intensive care unit (ICU). Despite advances in understanding the underlying pathophysiology, evidence for specific immunomodulatory treatment does not exist to date. Therapeutic plasma exchange (TPE) represents an adjunctive treatment approach to rebalance immune homeostasis. In the EXCHANGE-1 trial, we recently demonstrated a rapid hemodynamic improvement, possibly caused by the removal of harmful mediators and the replacement of protective plasma proteins. The aim of this secondary analysis is to further characterize the underlying immunomodulatory effects and to identify biomarkers that may predict treatment response.
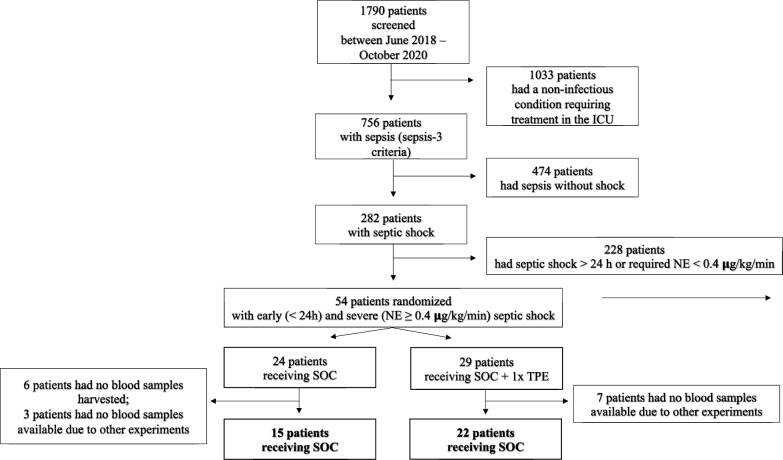
Methods: This secondary analysis included patients in early septic shock (< 24 h duration) and a norepinephrine (NE) dose of ≥ 0.4 μg/kg/min. Patients were randomized 1:1 to receive standard of care (SOC) or SOC + one single TPE and plasma samples were collected before and after TPE. Within-group and between group effects of circulating levels of acute-phase proteins [CRP and Pentraxin3 (PTX3)], inflammatory mediators (IL-4, IL-6, IL-8, IL-10, TNF-α, IL-2Rα/CD25) and damage-associated molecular pattern (DAMP) [cell-free DNA (cfDNA)] were analyzed via paired t test or Wilcoxon signed-rank test and a mixed-effects model. Multivariate mixed-effects modeling of NE and lactate reduction was performed to investigate if cfDNA could be associated with treatment response to TPE.
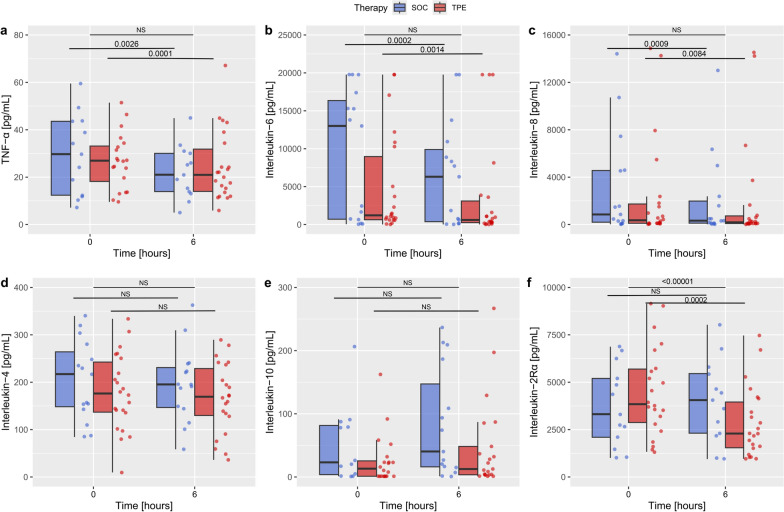
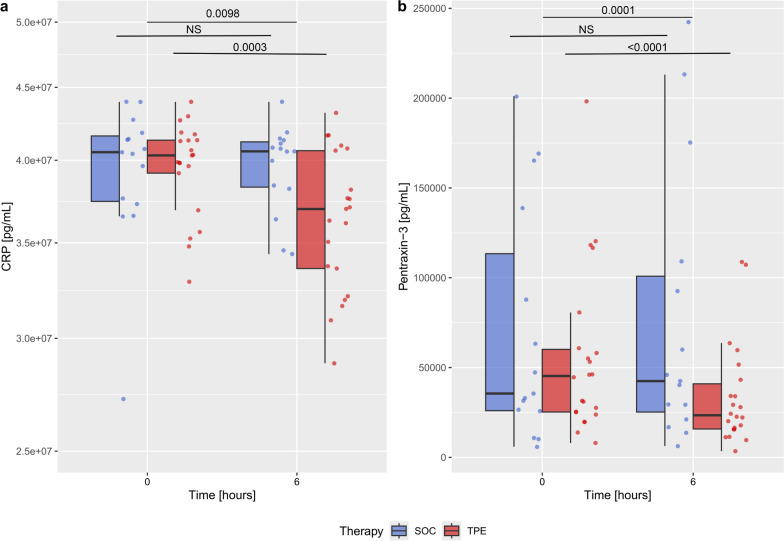
Results: TPE led to a significant reduction in circulating acute-phase protein levels (CRP p = 0.00976, PTX3 p = 0.0001). Pro-inflammatory cytokines, such as circulating TNF-α-, IL-6- und IL-8-levels, were significantly reduced in both groups with no significant difference between treatment groups except for IL-2Rα/CD25 (p ≤ 0.0001). In a multivariate mixed-effects model, rising cfDNA levels over the first 6 h indicated refractoriness to SOC treatment regarding NE (p = 0.004) and lactate (p = 0.001), whereas those receiving TPE demonstrated sustained reductions in both parameters.
Conclusions: In this secondary analysis of the EXCHANGE-1 trial adjunctive TPE is associated with the reduction of acute-phase proteins and IL-2Rα/CD25, however not with the reduction of pro-inflammatory cytokines. This phenomenon could contribute to the observed enhancement in hemodynamics among patients with septic shock. Furthermore, TPE may be particularly beneficial for patients with septic shock who exhibit rising levels of cfDNA.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
