Andrea Soosaipillai, Inbar Nardi-Agmon, Davor Brinc, Anselmo Fabros, Peter A Kavsak, Paaladinesh Thavendiranathan, Ashley Di Meo
{"title":"Macrotroponin interference and association with cardiotoxicity in patients receiving cardiotoxic breast cancer therapy: a pilot study.","authors":"Andrea Soosaipillai, Inbar Nardi-Agmon, Davor Brinc, Anselmo Fabros, Peter A Kavsak, Paaladinesh Thavendiranathan, Ashley Di Meo","doi":"10.1186/s40959-025-00314-9","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Cancer therapy-related cardiac dysfunction (CTRCD) is an important adverse effect in patients receiving potential cardiotoxic cancer therapies. Interpretation of cardiac troponin results can be affected by presence of macrotroponin, which can complicate CTRCD assessment. We aimed to assess whether macrotroponin is detectable in women with ERBB2 + breast cancer receiving sequential therapy with anthracyclines and trastuzumab.</p><p><strong>Methods: </strong>A total of 20 serum samples from 12 ERBB2 + breast cancer patients (median age: 55 years, range: 30-69 years) who exhibited a significant increase in high-sensitivity cardiac troponin I (hs-cTnI) from baseline to post-anthracycline (~ 2 months after therapy initiation) and/or 3-months into trastuzumab therapy (~ 5 months after therapy initiation) and/or who had at least one hs-cTnI value above the female-specific 99th percentile (hs-cTnI > 16 ng/L) and had available banked blood for analysis were included in this pilot study. Samples were analyzed using the Abbott STAT High-Sensitive Troponin-I and Roche Elecsys Troponin T hs STAT assays. Macrotroponin was detected by treating the sample with protein G and re-measuring hs-cTn. Macrotroponin presence was defined as a hs-cTnI or hs-cTnT recovery of < 40% or 85%, respectively.</p><p><strong>Results: </strong>Macrotroponin was not identified after anthracycline treatment but was present in four patients 3-months into trastuzumab therapy, two of which had hs-cTnI concentrations above the 99th percentile. None of these patients exhibited a significant reduction in LVEF and/or GLS despite having significant elevations in hs-cTnI.</p><p><strong>Conclusions: </strong>Clinicians should be cautious of benign hs-cTn elevations resulting from macrotroponin presence, as it can complicate CTRCD assessment.</p>","PeriodicalId":9804,"journal":{"name":"Cardio-oncology","volume":"11 1","pages":"18"},"PeriodicalIF":3.2000,"publicationDate":"2025-02-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11827144/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardio-oncology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40959-025-00314-9","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Cancer therapy-related cardiac dysfunction (CTRCD) is an important adverse effect in patients receiving potential cardiotoxic cancer therapies. Interpretation of cardiac troponin results can be affected by presence of macrotroponin, which can complicate CTRCD assessment. We aimed to assess whether macrotroponin is detectable in women with ERBB2 + breast cancer receiving sequential therapy with anthracyclines and trastuzumab.
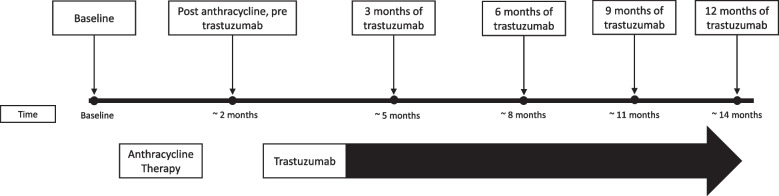
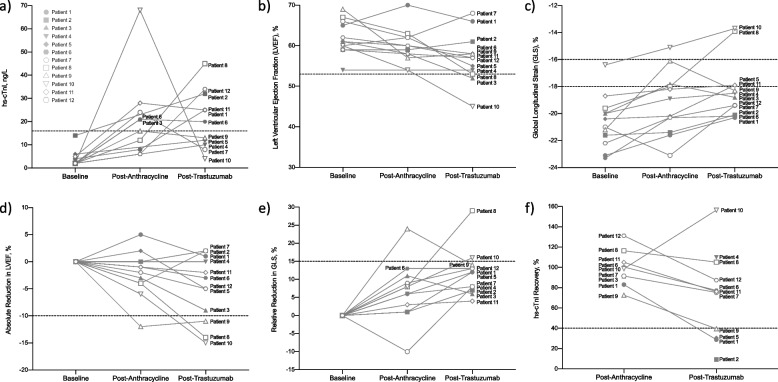
Methods: A total of 20 serum samples from 12 ERBB2 + breast cancer patients (median age: 55 years, range: 30-69 years) who exhibited a significant increase in high-sensitivity cardiac troponin I (hs-cTnI) from baseline to post-anthracycline (~ 2 months after therapy initiation) and/or 3-months into trastuzumab therapy (~ 5 months after therapy initiation) and/or who had at least one hs-cTnI value above the female-specific 99th percentile (hs-cTnI > 16 ng/L) and had available banked blood for analysis were included in this pilot study. Samples were analyzed using the Abbott STAT High-Sensitive Troponin-I and Roche Elecsys Troponin T hs STAT assays. Macrotroponin was detected by treating the sample with protein G and re-measuring hs-cTn. Macrotroponin presence was defined as a hs-cTnI or hs-cTnT recovery of < 40% or 85%, respectively.
Results: Macrotroponin was not identified after anthracycline treatment but was present in four patients 3-months into trastuzumab therapy, two of which had hs-cTnI concentrations above the 99th percentile. None of these patients exhibited a significant reduction in LVEF and/or GLS despite having significant elevations in hs-cTnI.
Conclusions: Clinicians should be cautious of benign hs-cTn elevations resulting from macrotroponin presence, as it can complicate CTRCD assessment.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
