Adam Strzelczyk, Felix von Podewils, Hajo M Hamer, Susanne Knake, Felix Rosenow, Kerstin Alexandra Klotz, Gerhard Kurlemann, Nico Melzer, Elisa Buhleier, Catrin Mann, Laurent M Willems, Johann Philipp Zöllner, Bernadette Gaida, Jeanne Cuny, David Bellaire, Ilka Immisch, Leena Kämppi, Andreas Brunklaus, Susanne Schubert-Bast
{"title":"Post-marketing Experience with Cenobamate in the Treatment of Focal Epilepsies: A Multicentre Cohort Study.","authors":"Adam Strzelczyk, Felix von Podewils, Hajo M Hamer, Susanne Knake, Felix Rosenow, Kerstin Alexandra Klotz, Gerhard Kurlemann, Nico Melzer, Elisa Buhleier, Catrin Mann, Laurent M Willems, Johann Philipp Zöllner, Bernadette Gaida, Jeanne Cuny, David Bellaire, Ilka Immisch, Leena Kämppi, Andreas Brunklaus, Susanne Schubert-Bast","doi":"10.1007/s40263-025-01158-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>In randomised controlled trials, adjunctive cenobamate (CNB) has been shown to reduce seizure frequency in patients with drug-resistant focal epilepsy. Studies conducted in real-world settings provide valuable complementary data to further characterise the drug's profile.</p><p><strong>Objective: </strong>To assess the efficacy, retention and tolerability of adjunctive cenobamate (CNB), and to identify factors that might predict these outcomes in the clinical treatment of focal epilepsies.</p><p><strong>Methods: </strong>This multicentre, retrospective cohort study included all patients who began CNB treatment between October 2020 and April 2023 at seven participating epilepsy centres. Baseline and follow-up data were collected from patients' medical records, covering clinical characteristics and outcome data such as seizure frequency, dosing of CNB, physician-assessed Clinical Global Impression of Change, treatment-emergent adverse events (TEAEs), CNB retention and reasons for discontinuation.</p><p><strong>Results: </strong>A total of 234 patients [mean age 40.7 ± 14 years, median 40 years, range 11-82 years; five adolescents under 18 years; 99 (42.3%) males] were analysed. The mean epilepsy duration at study entry was 23.2 ± 14.5 years (median 21 years, range 0.75-63 years), with the average age of epilepsy onset being 17.5 ± 13.0 years (median 17 years, range 0.1-71 years). The patients were taking a mean of 2.6 ± 0.8 (median 3) anti-seizure medications (ASMs) before starting CNB, and had failed a mean of 6 ± 3.3 (median 6) of further ASMs in the past. CNB exposure ranged from 5 to 1162 days, amounting to a total exposure time of 264.7 years. The retention rate was 92.6% at 3 months, 87.2% at 6 months and 77.8% at 12 months. At 3 months, 52.6% achieved a 50% seizure reduction, with 14.5% reporting seizure freedom; by 12 months, 47.7% maintained a 50% response rate and 11.9% were seizure-free. No significant differences in responder rates were observed based on sex, aetiology, seizure localisation, number of ASMs or target dose. The mean maximum CNB dose was 236.7 ± 97.4 mg (median 200 mg, range 12.5-450 mg), with 28 patients (12.0%) titrated up to 400 mg or above. During CNB treatment, 43.6% of patients were able to discontinue, and a further 24.4% were able to reduce the dose of a concomitant ASM. During CNB treatment, 144 patients (61.5%) experienced TEAEs. The most common TEAEs were sedation (n = 84, 35.9%), dizziness (n = 58, 24.8%) and ataxia (n = 23, 9.8%).</p><p><strong>Conclusions: </strong>CNB showed a relatively high and clinically useful 50% responder rate of 47.7% and an overall retention of 77.8% at 1 year. We were unable to identify specific predictors for response and retention, indicating that CNB may be beneficial for patients with a history of multiple failed ASMs, a high number of concomitant ASMs and any localisation or aetiology of focal epilepsy.</p>","PeriodicalId":10508,"journal":{"name":"CNS drugs","volume":" ","pages":"321-331"},"PeriodicalIF":7.0000,"publicationDate":"2025-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11850496/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"CNS drugs","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s40263-025-01158-8","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/2/15 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: In randomised controlled trials, adjunctive cenobamate (CNB) has been shown to reduce seizure frequency in patients with drug-resistant focal epilepsy. Studies conducted in real-world settings provide valuable complementary data to further characterise the drug's profile.
Objective: To assess the efficacy, retention and tolerability of adjunctive cenobamate (CNB), and to identify factors that might predict these outcomes in the clinical treatment of focal epilepsies.
Methods: This multicentre, retrospective cohort study included all patients who began CNB treatment between October 2020 and April 2023 at seven participating epilepsy centres. Baseline and follow-up data were collected from patients' medical records, covering clinical characteristics and outcome data such as seizure frequency, dosing of CNB, physician-assessed Clinical Global Impression of Change, treatment-emergent adverse events (TEAEs), CNB retention and reasons for discontinuation.
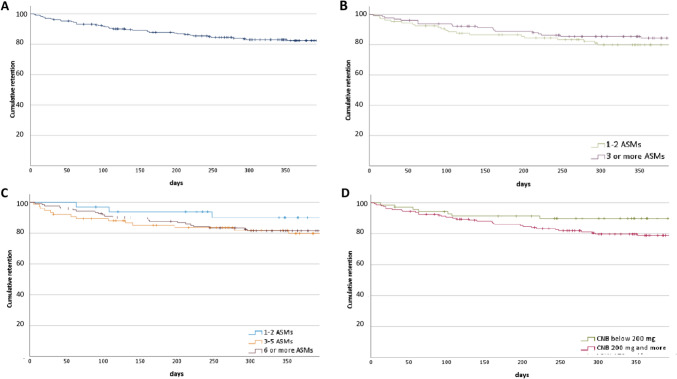
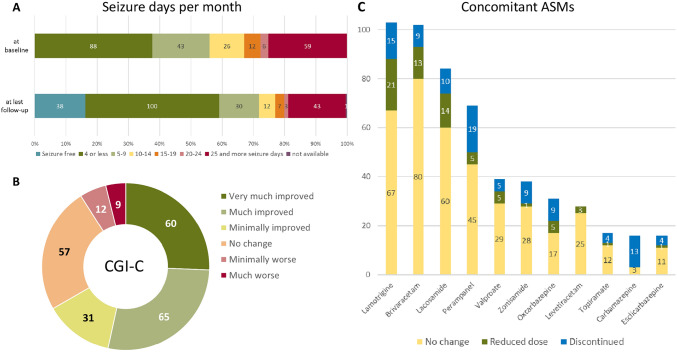
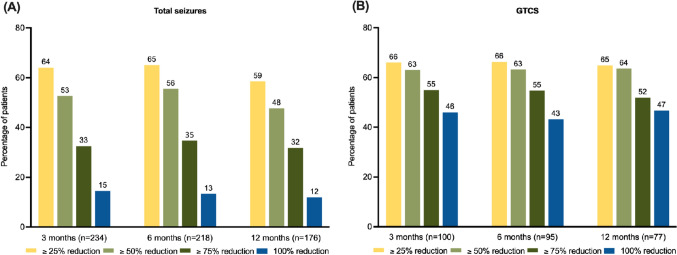
Results: A total of 234 patients [mean age 40.7 ± 14 years, median 40 years, range 11-82 years; five adolescents under 18 years; 99 (42.3%) males] were analysed. The mean epilepsy duration at study entry was 23.2 ± 14.5 years (median 21 years, range 0.75-63 years), with the average age of epilepsy onset being 17.5 ± 13.0 years (median 17 years, range 0.1-71 years). The patients were taking a mean of 2.6 ± 0.8 (median 3) anti-seizure medications (ASMs) before starting CNB, and had failed a mean of 6 ± 3.3 (median 6) of further ASMs in the past. CNB exposure ranged from 5 to 1162 days, amounting to a total exposure time of 264.7 years. The retention rate was 92.6% at 3 months, 87.2% at 6 months and 77.8% at 12 months. At 3 months, 52.6% achieved a 50% seizure reduction, with 14.5% reporting seizure freedom; by 12 months, 47.7% maintained a 50% response rate and 11.9% were seizure-free. No significant differences in responder rates were observed based on sex, aetiology, seizure localisation, number of ASMs or target dose. The mean maximum CNB dose was 236.7 ± 97.4 mg (median 200 mg, range 12.5-450 mg), with 28 patients (12.0%) titrated up to 400 mg or above. During CNB treatment, 43.6% of patients were able to discontinue, and a further 24.4% were able to reduce the dose of a concomitant ASM. During CNB treatment, 144 patients (61.5%) experienced TEAEs. The most common TEAEs were sedation (n = 84, 35.9%), dizziness (n = 58, 24.8%) and ataxia (n = 23, 9.8%).
Conclusions: CNB showed a relatively high and clinically useful 50% responder rate of 47.7% and an overall retention of 77.8% at 1 year. We were unable to identify specific predictors for response and retention, indicating that CNB may be beneficial for patients with a history of multiple failed ASMs, a high number of concomitant ASMs and any localisation or aetiology of focal epilepsy.
期刊介绍:
CNS Drugs promotes rational pharmacotherapy within the disciplines of clinical psychiatry and neurology. The Journal includes:
- Overviews of contentious or emerging issues.
- Comprehensive narrative reviews that provide an authoritative source of information on pharmacological approaches to managing neurological and psychiatric illnesses.
- Systematic reviews that collate empirical evidence to answer a specific research question, using explicit, systematic methods as outlined by the PRISMA statement.
- Adis Drug Reviews of the properties and place in therapy of both newer and established drugs in neurology and psychiatry.
- Original research articles reporting the results of well-designed studies with a strong link to clinical practice, such as clinical pharmacodynamic and pharmacokinetic studies, clinical trials, meta-analyses, outcomes research, and pharmacoeconomic and pharmacoepidemiological studies.
Additional digital features (including animated abstracts, video abstracts, slide decks, audio slides, instructional videos, infographics, podcasts and animations) can be published with articles; these are designed to increase the visibility, readership and educational value of the journal’s content. In addition, articles published in CNS Drugs may be accompanied by plain language summaries to assist readers who have some knowledge of, but not in-depth expertise in, the area to understand important medical advances.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
