Implementing Cognitive Stimulation Therapy (CST) for Dementia in a Low-Resource Setting: A Case Study in Tanzania Exploring Barriers, Facilitators, and Recommendations for Practice.
Emily Fisher, Sarah Mkenda, Jessica Walker, Ssenku Safic, Charlotte R Stoner, Catherine Dotchin, Stella-Maria Paddick, Godrule Lyimo, Jane Rogathi, Maria Jelen, Matthew Breckons, Jane Fossey, Richard Walker, Aimee Spector
{"title":"Implementing Cognitive Stimulation Therapy (CST) for Dementia in a Low-Resource Setting: A Case Study in Tanzania Exploring Barriers, Facilitators, and Recommendations for Practice.","authors":"Emily Fisher, Sarah Mkenda, Jessica Walker, Ssenku Safic, Charlotte R Stoner, Catherine Dotchin, Stella-Maria Paddick, Godrule Lyimo, Jane Rogathi, Maria Jelen, Matthew Breckons, Jane Fossey, Richard Walker, Aimee Spector","doi":"10.1007/s43477-024-00142-6","DOIUrl":null,"url":null,"abstract":"<p><p>Cognitive Stimulation Therapy (CST) is a group psychosocial intervention for people with mild-to-moderate dementia. Despite evidence supporting its effectiveness, cost-effectiveness, and cultural adaptation internationally, CST has yet to be implemented in routine practice outside of the UK. This study consisted of multiple phases. In the first phase, we engaged stakeholders to explore the barriers and facilitators to CST implementation in Tanzania. In the second phase, we developed implementation strategies. In the third phase, we tested these strategies in a study of CST in a tertiary hospital in northern Tanzania. The Consolidated Framework for Implementation Research (CFIR) guided the study. We conducted stakeholder engagement with decision-makers, healthcare professionals, people with dementia and their family caregivers (<i>n</i> = 49) to identify barriers and facilitators to implementation. We developed an implementation plan that included 20 implementation strategies related to 12 CFIR constructs. Subsequently, we tested these strategies by running eight CST groups with 49 participants. In follow-up interviews with people with dementia, carers and healthcare professionals, we identified 18 key CFIR constructs as barriers or facilitators to successfully implementing CST. CST was compatible with the standards of care in a tertiary referral hospital in northern Tanzania. To implement CST in low-resource settings, we recommend running dementia awareness initiatives, screening for dementia in outpatients and community settings, developing a train-the-trainer model, employing a task-shifting approach, and creating a dementia-friendly space for dementia services. Our findings can inform future efforts to implement CST and other psychosocial interventions for dementia in low-resource settings.</p><p><strong>Supplementary information: </strong>The online version contains supplementary material available at 10.1007/s43477-024-00142-6.</p>","PeriodicalId":73165,"journal":{"name":"Global implementation research and applications","volume":"5 1","pages":"106-123"},"PeriodicalIF":0.0000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11821707/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Global implementation research and applications","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s43477-024-00142-6","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/11 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
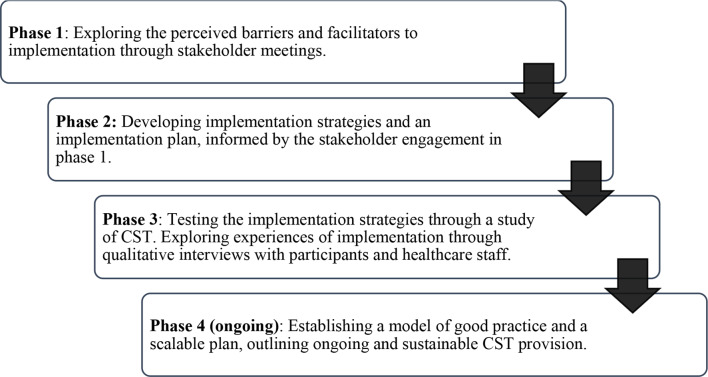
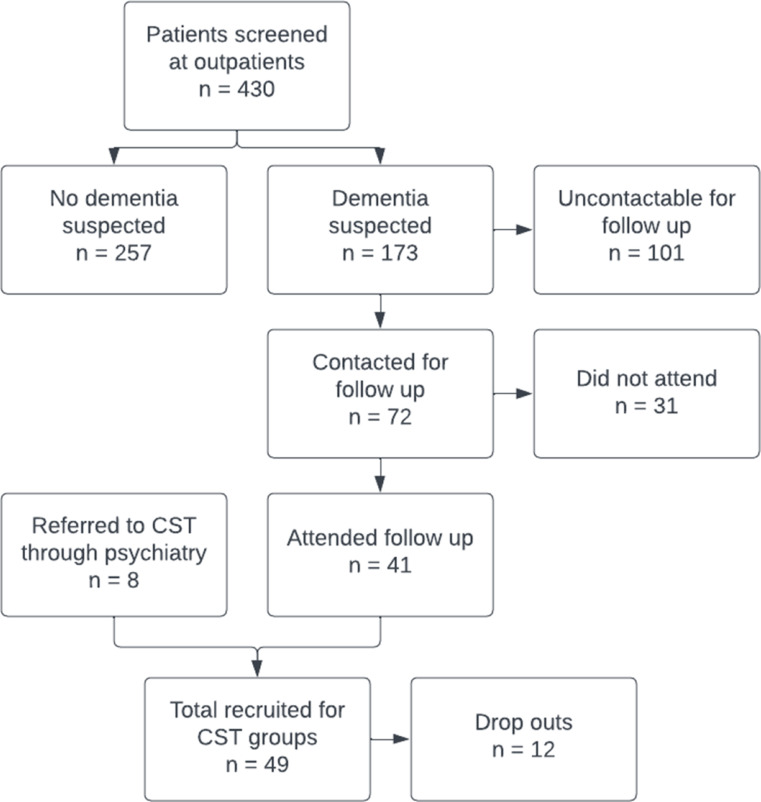
Cognitive Stimulation Therapy (CST) is a group psychosocial intervention for people with mild-to-moderate dementia. Despite evidence supporting its effectiveness, cost-effectiveness, and cultural adaptation internationally, CST has yet to be implemented in routine practice outside of the UK. This study consisted of multiple phases. In the first phase, we engaged stakeholders to explore the barriers and facilitators to CST implementation in Tanzania. In the second phase, we developed implementation strategies. In the third phase, we tested these strategies in a study of CST in a tertiary hospital in northern Tanzania. The Consolidated Framework for Implementation Research (CFIR) guided the study. We conducted stakeholder engagement with decision-makers, healthcare professionals, people with dementia and their family caregivers (n = 49) to identify barriers and facilitators to implementation. We developed an implementation plan that included 20 implementation strategies related to 12 CFIR constructs. Subsequently, we tested these strategies by running eight CST groups with 49 participants. In follow-up interviews with people with dementia, carers and healthcare professionals, we identified 18 key CFIR constructs as barriers or facilitators to successfully implementing CST. CST was compatible with the standards of care in a tertiary referral hospital in northern Tanzania. To implement CST in low-resource settings, we recommend running dementia awareness initiatives, screening for dementia in outpatients and community settings, developing a train-the-trainer model, employing a task-shifting approach, and creating a dementia-friendly space for dementia services. Our findings can inform future efforts to implement CST and other psychosocial interventions for dementia in low-resource settings.
Supplementary information: The online version contains supplementary material available at 10.1007/s43477-024-00142-6.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
