Evaluating the prognostic significance of tumor deposits in gastric cancer and strategies for their integration into the TNM staging system: a single-center retrospective study.
Jun Yu, Ruirong Yao, Ning Han, Linbin Lu, Ling Chen, Abudurousuli Reyila, Xinlin Wang, Junya Yan, Shibo Wang, Yong Guo, Qingchuan Zhao, Kaichun Wu, Yuanyuan Lu, Gang Ji, Zengshan Li, Xianchun Gao, Yongzhan Nie
{"title":"Evaluating the prognostic significance of tumor deposits in gastric cancer and strategies for their integration into the TNM staging system: a single-center retrospective study.","authors":"Jun Yu, Ruirong Yao, Ning Han, Linbin Lu, Ling Chen, Abudurousuli Reyila, Xinlin Wang, Junya Yan, Shibo Wang, Yong Guo, Qingchuan Zhao, Kaichun Wu, Yuanyuan Lu, Gang Ji, Zengshan Li, Xianchun Gao, Yongzhan Nie","doi":"10.1007/s13402-025-01046-9","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>To propose a new optimal strategy for incorporating tumor deposit (TD) into TNM staging.</p><p><strong>Methods: </strong>Totally, 2730 consecutive gastric cancer (GC) patients were included according to the presence and count of TDs between January 2011 and December 2014. Overall survival (OS) was analyzed using Cox regression and propensity score matching (PSM). The relationship between the number of TDs and GC patients' prognosis was analyzed using restricted cubic spline curves and compared with the prognostic value of lymph node metastases (LNMs). Harrell's C-index (C-index) and the Akaike information criterion (AIC) were employed to assess the prognostic performance of different staging systems.</p><p><strong>Results: </strong>The positive rate of TD was 9.67% (264/2730). The presence of TD was associated with poorer OS before PSM (hazard ratio (HR): 3.31; 95% confidence interval (CI): 2.84, 3.85) and after PSM (HR: 1.62; 95%CI: 1.31, 2.00). The modified TNM staging, equating one TD to four LNMs, achieved superior prognostic performance, surpassing the 8th edition AJCC TNM staging and other modified systems (C-index: 0.751, AIC: 15954.0). In this system, 12.04% (26/216) of TD-positive patients were upstaged from stage II to stage III. These upstaged patients had worse outcomes than the remaining stage II patients (HR: 10.97; 95% CI: 4.55-26.44), while outcomes were similar to those of original stage III patients (HR:1.08; 95%CI: 0.66, 1.78).</p><p><strong>Conclusion: </strong>The presence and increased number of TDs were noted to be associated with GC patients' poor prognosis. Integrating TD count with LNMs could enhance the prognostic accuracy of the TNM staging system.</p>","PeriodicalId":9690,"journal":{"name":"Cellular Oncology","volume":" ","pages":"761-773"},"PeriodicalIF":4.8000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12119653/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cellular Oncology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s13402-025-01046-9","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/2/17 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: To propose a new optimal strategy for incorporating tumor deposit (TD) into TNM staging.
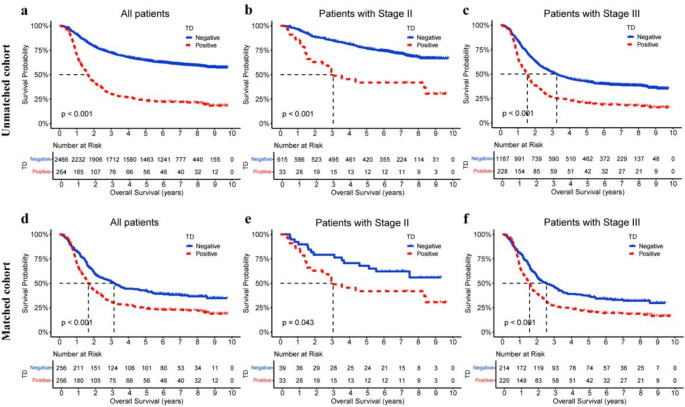
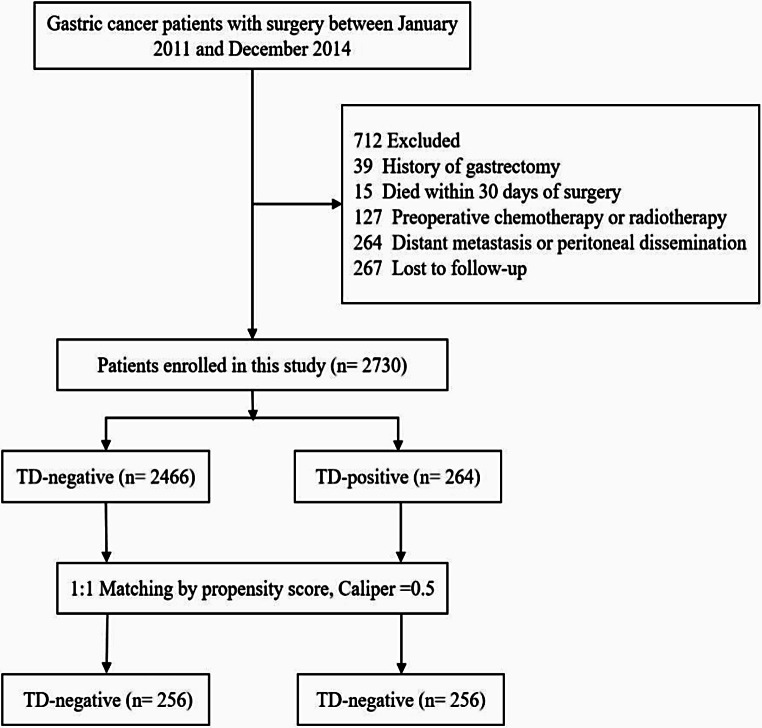
Methods: Totally, 2730 consecutive gastric cancer (GC) patients were included according to the presence and count of TDs between January 2011 and December 2014. Overall survival (OS) was analyzed using Cox regression and propensity score matching (PSM). The relationship between the number of TDs and GC patients' prognosis was analyzed using restricted cubic spline curves and compared with the prognostic value of lymph node metastases (LNMs). Harrell's C-index (C-index) and the Akaike information criterion (AIC) were employed to assess the prognostic performance of different staging systems.
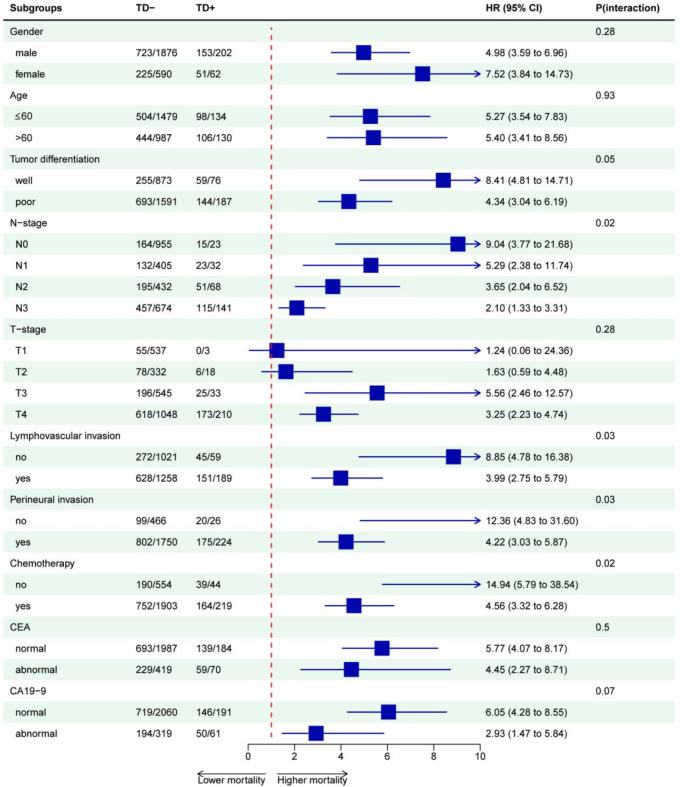
Results: The positive rate of TD was 9.67% (264/2730). The presence of TD was associated with poorer OS before PSM (hazard ratio (HR): 3.31; 95% confidence interval (CI): 2.84, 3.85) and after PSM (HR: 1.62; 95%CI: 1.31, 2.00). The modified TNM staging, equating one TD to four LNMs, achieved superior prognostic performance, surpassing the 8th edition AJCC TNM staging and other modified systems (C-index: 0.751, AIC: 15954.0). In this system, 12.04% (26/216) of TD-positive patients were upstaged from stage II to stage III. These upstaged patients had worse outcomes than the remaining stage II patients (HR: 10.97; 95% CI: 4.55-26.44), while outcomes were similar to those of original stage III patients (HR:1.08; 95%CI: 0.66, 1.78).
Conclusion: The presence and increased number of TDs were noted to be associated with GC patients' poor prognosis. Integrating TD count with LNMs could enhance the prognostic accuracy of the TNM staging system.
Cellular OncologyBiochemistry, Genetics and Molecular Biology-Cancer Research
CiteScore
10.40
自引率
1.50%
发文量
0
审稿时长
16 weeks
期刊介绍:
The Official Journal of the International Society for Cellular Oncology
Focuses on translational research
Addresses the conversion of cell biology to clinical applications
Cellular Oncology publishes scientific contributions from various biomedical and clinical disciplines involved in basic and translational cancer research on the cell and tissue level, technical and bioinformatics developments in this area, and clinical applications. This includes a variety of fields like genome technology, micro-arrays and other high-throughput techniques, genomic instability, SNP, DNA methylation, signaling pathways, DNA organization, (sub)microscopic imaging, proteomics, bioinformatics, functional effects of genomics, drug design and development, molecular diagnostics and targeted cancer therapies, genotype-phenotype interactions.
A major goal is to translate the latest developments in these fields from the research laboratory into routine patient management. To this end Cellular Oncology forms a platform of scientific information exchange between molecular biologists and geneticists, technical developers, pathologists, (medical) oncologists and other clinicians involved in the management of cancer patients.
In vitro studies are preferentially supported by validations in tumor tissue with clinicopathological associations.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
