{"title":"A low preoperative platelet-to-white blood cell ratio is associated with acute kidney injury following cerebral aneurysm treatment in South Korea.","authors":"Seung-Woon Lim, Woo-Young Jo, Hee-Pyoung Park","doi":"10.4266/acc.003120","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Inflammation is involved in the pathophysiology of postoperative acute kidney injury (AKI). We investigated whether preoperative platelet-to-white blood cell ratio (PWR), a novel serum biomarker of systemic inflammation, was associated with postoperative AKI following cerebral aneurysm treatment. We also compared the discrimination power of preoperative PWR with those of other preoperative systemic inflammatory indices in predicting postoperative AKI.</p><p><strong>Methods: </strong>Perioperative data including preoperative systemic inflammatory indices and cerebral aneurysm-related variables were retrospectively analyzed in 4,429 cerebral aneurysm patients undergoing surgical clipping or endovascular coiling. Based on the cutoff value of preoperative PWR, patients were divided into the high PWR (≥39.04, n=1,924) and low PWR (<39.04, n=2,505) groups. After propensity score matching (PSM), 1,168 patients in each group were included in the data analysis. AKI was defined according to the Kidney Disease Improving Global Outcomes guidelines.</p><p><strong>Results: </strong>Postoperative AKI occurred more frequently in the low PWR group than in the high PWR group before PSM (45 [1.8%] vs. 7 [0.4%], P<0.001) and after (17 [1.5%] vs. 5 [0.4%], P=0.016). A low preoperative PWR was predictive of postoperative AKI before PSM (odds ratio [95% CI], 3.93 [1.74-8.87]; P<0.001) and after (3.44 [1.26-9.34], P=0.016). Preoperative PWR showed the highest area under the curve for postoperative AKI (0.713 [0.644-0.782], P<0.001), followed by preoperative platelet-to-neutrophil ratio (0.694 [0.619-0.769], P<0.001), neutrophil percentage-to-albumin ratio (0.671 [0.592-0.750], P<0.001), white blood cell-to-hemoglobin ratio (0.665 [0.579-0.750], P<0.001), neutrophil-to-lymphocyte ratio (0.648 [0.569-0.728], P<0.001), and systemic inflammatory index (0.615 [0.532-0.698], P=0.004).</p><p><strong>Conclusions: </strong>A low preoperative PWR was associated with postoperative AKI following cerebral aneurysm treatment.</p>","PeriodicalId":44118,"journal":{"name":"Acute and Critical Care","volume":" ","pages":"59-68"},"PeriodicalIF":2.0000,"publicationDate":"2025-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11924346/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Acute and Critical Care","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4266/acc.003120","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/2/21 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Inflammation is involved in the pathophysiology of postoperative acute kidney injury (AKI). We investigated whether preoperative platelet-to-white blood cell ratio (PWR), a novel serum biomarker of systemic inflammation, was associated with postoperative AKI following cerebral aneurysm treatment. We also compared the discrimination power of preoperative PWR with those of other preoperative systemic inflammatory indices in predicting postoperative AKI.
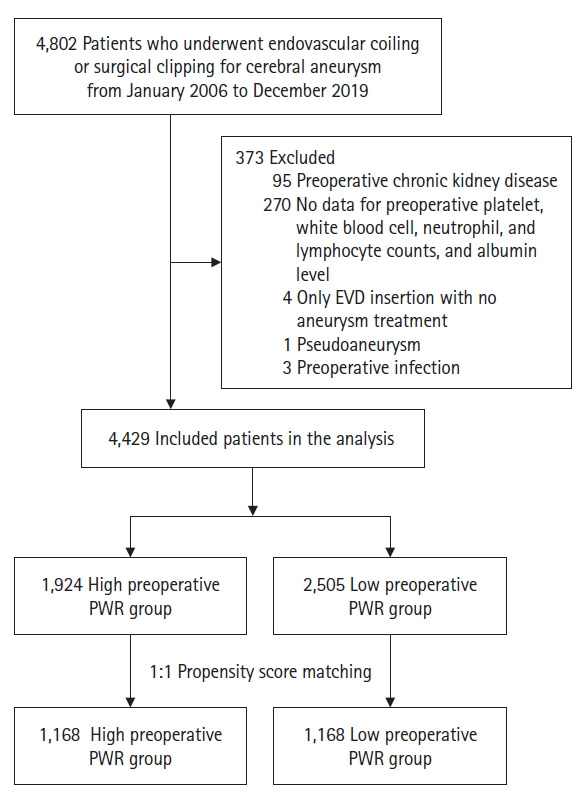
Methods: Perioperative data including preoperative systemic inflammatory indices and cerebral aneurysm-related variables were retrospectively analyzed in 4,429 cerebral aneurysm patients undergoing surgical clipping or endovascular coiling. Based on the cutoff value of preoperative PWR, patients were divided into the high PWR (≥39.04, n=1,924) and low PWR (<39.04, n=2,505) groups. After propensity score matching (PSM), 1,168 patients in each group were included in the data analysis. AKI was defined according to the Kidney Disease Improving Global Outcomes guidelines.
Results: Postoperative AKI occurred more frequently in the low PWR group than in the high PWR group before PSM (45 [1.8%] vs. 7 [0.4%], P<0.001) and after (17 [1.5%] vs. 5 [0.4%], P=0.016). A low preoperative PWR was predictive of postoperative AKI before PSM (odds ratio [95% CI], 3.93 [1.74-8.87]; P<0.001) and after (3.44 [1.26-9.34], P=0.016). Preoperative PWR showed the highest area under the curve for postoperative AKI (0.713 [0.644-0.782], P<0.001), followed by preoperative platelet-to-neutrophil ratio (0.694 [0.619-0.769], P<0.001), neutrophil percentage-to-albumin ratio (0.671 [0.592-0.750], P<0.001), white blood cell-to-hemoglobin ratio (0.665 [0.579-0.750], P<0.001), neutrophil-to-lymphocyte ratio (0.648 [0.569-0.728], P<0.001), and systemic inflammatory index (0.615 [0.532-0.698], P=0.004).
Conclusions: A low preoperative PWR was associated with postoperative AKI following cerebral aneurysm treatment.
背景:炎症与术后急性肾损伤(AKI)的病理生理学有关。我们研究了术前血小板与白细胞比值(PWR)这一新型全身炎症血清生物标记物是否与脑动脉瘤治疗术后急性肾损伤相关。我们还比较了术前PWR与其他术前全身炎症指标在预测术后AKI方面的鉴别力:方法:我们回顾性分析了4429名接受手术夹闭或血管内旋转治疗的脑动脉瘤患者的围手术期数据,包括术前全身炎症指数和脑动脉瘤相关变量。根据术前脉搏波速度的临界值,将患者分为高脉搏波速度组(≥39.04,n=1,924)和低脉搏波速度组(PWR≥39.04,n=1,924):在 PSM 之前,低脉搏波速度组比高脉搏波速度组更容易发生术后 AKI(45 [1.8%] vs. 7 [0.4%],PConclusions:术前脉搏波速度低与脑动脉瘤治疗术后 AKI 有关。



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
