Jaeyoung Choi, Song-Hee Kim, Ryoung-Eun Ko, Gee Young Suh, Jeong Hoon Yang, Chi-Min Park, Joongbum Cho, Chi Ryang Chung
{"title":"Simulating the effects of reducing transfer latency from the intensive care unit on intensive care unit bed utilization in a Korean Tertiary Hospital.","authors":"Jaeyoung Choi, Song-Hee Kim, Ryoung-Eun Ko, Gee Young Suh, Jeong Hoon Yang, Chi-Min Park, Joongbum Cho, Chi Ryang Chung","doi":"10.4266/acc.002976","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Latency in transferring patients from intensive care units (ICUs) to general wards impedes the optimal allocation of ICU resources, underscoring the urgency of initiatives to reduce it. This study evaluates the extent of ICU transfer latency and assesses the potential benefits of minimizing it.</p><p><strong>Methods: </strong>Transfer latency was measured as the time between the first transfer request and the actual ICU discharge at a single-center tertiary hospital in 2021. Computer-based simulations and cost analyses were performed to examine how reducing transfer latency could affect average hourly ICU bed occupancy, the proportion of time ICU occupancy exceeds 80%, and hospital costs. The first analysis evaluated all ICU admissions, and the second analysis targeted a subset of ICU admissions with longer transfer latency, those requiring infectious precautions.</p><p><strong>Results: </strong>A total of 7,623 ICU admissions were analyzed, and the median transfer latency was 5.7 hours. Eliminating transfer latency for all ICU admissions would have resulted in a 32.8% point decrease in the proportion of time ICU occupancy exceeded 80%, and a potential annual savings of $6.18 million. Eliminating transfer latency for patients under infectious precautions would have decreased the time ICU occupancy exceeded 80% by 13.5% points, and reduced annual costs by a potential $1.26 million.</p><p><strong>Conclusions: </strong>Transfer latency from ICUs to general wards might contribute to high ICU occupancy. Efforts to minimize latency for all admissions, or even for a subset of admissions with particularly long transfer latency, could enable more efficient use of ICU resources.</p>","PeriodicalId":44118,"journal":{"name":"Acute and Critical Care","volume":" ","pages":"18-28"},"PeriodicalIF":2.0000,"publicationDate":"2025-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11924396/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Acute and Critical Care","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4266/acc.002976","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/2/21 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Latency in transferring patients from intensive care units (ICUs) to general wards impedes the optimal allocation of ICU resources, underscoring the urgency of initiatives to reduce it. This study evaluates the extent of ICU transfer latency and assesses the potential benefits of minimizing it.
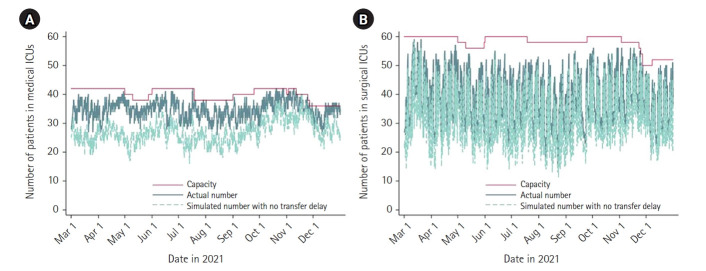
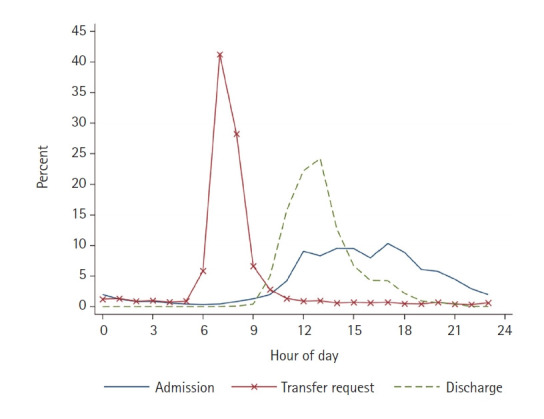
Methods: Transfer latency was measured as the time between the first transfer request and the actual ICU discharge at a single-center tertiary hospital in 2021. Computer-based simulations and cost analyses were performed to examine how reducing transfer latency could affect average hourly ICU bed occupancy, the proportion of time ICU occupancy exceeds 80%, and hospital costs. The first analysis evaluated all ICU admissions, and the second analysis targeted a subset of ICU admissions with longer transfer latency, those requiring infectious precautions.
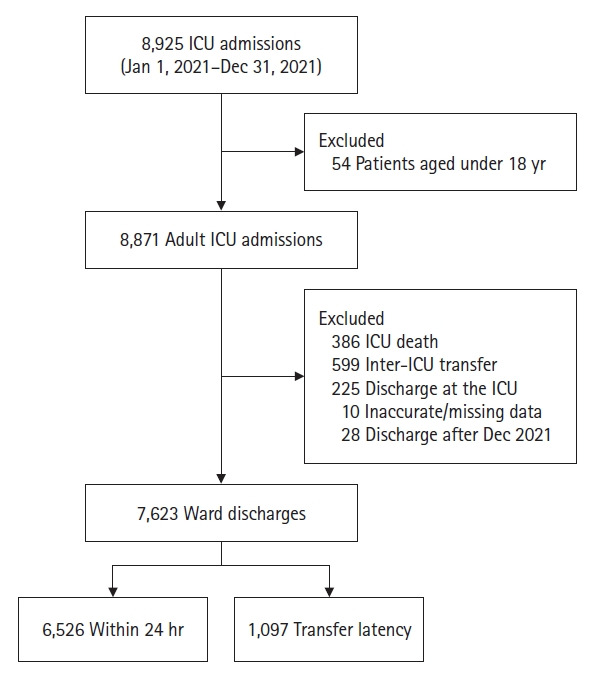
Results: A total of 7,623 ICU admissions were analyzed, and the median transfer latency was 5.7 hours. Eliminating transfer latency for all ICU admissions would have resulted in a 32.8% point decrease in the proportion of time ICU occupancy exceeded 80%, and a potential annual savings of $6.18 million. Eliminating transfer latency for patients under infectious precautions would have decreased the time ICU occupancy exceeded 80% by 13.5% points, and reduced annual costs by a potential $1.26 million.
Conclusions: Transfer latency from ICUs to general wards might contribute to high ICU occupancy. Efforts to minimize latency for all admissions, or even for a subset of admissions with particularly long transfer latency, could enable more efficient use of ICU resources.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
