Rahul Banerjee, Amber R. Fritz, Othman S. Akhtar, Ciara L. Freeman, Andrew J. Cowan, Nina Shah, Heather J. Landau, Shaji K. Kumar, Dan T. Vogl, Yvonne A. Efebera, Philip L. McCarthy, David H. Vesole, Adam Mendizabal, Amrita Y. Krishnan, George Somlo, Edward A. Stadtmauer, Marcelo C. Pasquini
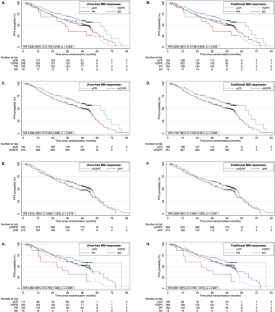
{"title":"Urine-free response criteria predict progression-free survival in multiple myeloma: a post hoc analysis of BMT CTN 0702","authors":"Rahul Banerjee, Amber R. Fritz, Othman S. Akhtar, Ciara L. Freeman, Andrew J. Cowan, Nina Shah, Heather J. Landau, Shaji K. Kumar, Dan T. Vogl, Yvonne A. Efebera, Philip L. McCarthy, David H. Vesole, Adam Mendizabal, Amrita Y. Krishnan, George Somlo, Edward A. Stadtmauer, Marcelo C. Pasquini","doi":"10.1038/s41375-025-02534-5","DOIUrl":null,"url":null,"abstract":"","PeriodicalId":18109,"journal":{"name":"Leukemia","volume":"39 4","pages":"1001-1004"},"PeriodicalIF":13.4000,"publicationDate":"2025-02-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Leukemia","FirstCategoryId":"3","ListUrlMain":"https://www.nature.com/articles/s41375-025-02534-5","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEMATOLOGY","Score":null,"Total":0}
期刊介绍:
Title: Leukemia
Journal Overview:
Publishes high-quality, peer-reviewed research
Covers all aspects of research and treatment of leukemia and allied diseases
Includes studies of normal hemopoiesis due to comparative relevance
Topics of Interest:
Oncogenes
Growth factors
Stem cells
Leukemia genomics
Cell cycle
Signal transduction
Molecular targets for therapy
And more
Content Types:
Original research articles
Reviews
Letters
Correspondence
Comments elaborating on significant advances and covering topical issues




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
