Carlos H Arteaga Duarte, Michel L Peters, Michelle H M de Goeij, Roy Spijkerman, Maarten J Postma
{"title":"Cost-effectiveness of nirmatrelvir/ritonavir in COVID-19 patient groups at high risk for progression to severe COVID-19 in the Netherlands.","authors":"Carlos H Arteaga Duarte, Michel L Peters, Michelle H M de Goeij, Roy Spijkerman, Maarten J Postma","doi":"10.1186/s12962-025-00604-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Nirmatrelvir/ritonavir is indicated for the treatment of COVID-19 in symptomatic adults with increased risk for severe illness, not requiring supplemental oxygen yet. From a Dutch societal perspective, a cost-utility assessment of nirmatrelvir/ritonavir versus best supportive care (BSC) was conducted in three patient groups: (a) immunocompromised patients, (b) patients aged at least 60 years with one comorbidity, (c) patients aged at least 70 years. Groups were selected considering their relevance as high-risk groups, as described in Dutch and international guidelines and recommendations.</p><p><strong>Methods: </strong>A one-year decision-tree, estimating costs and outcomes associated with a COVID-19 infection was coupled to a lifetime two-state Markov component simulating subsequent life-time survival and quality of life. Effectiveness estimates, informing the intervention preventing hospital admission or death, were based on real-world evidence by Lewnard and colleagues (2023) in a vaccinated population during a timeframe with predominance of the Omicron variant. Epidemiology relies on publicly available data, primarily sourced during the Omicron variant's era. In the decision tree, clinically relevant event-related disutilities per disease course were applied to adjusted age-dependent Dutch-specific utility levels. In the Markov component, a disutility was considered for post-ICU patients. Costs rely on Dutch pharmacoeconomic guidelines and public data sources. The incremental cost-effectiveness ratio (ICER) was analysed as the main outcome, with a positive ICER indicating the cost associated with each additional quality-adjusted life year (QALY) gained by adopting the intervention.</p><p><strong>Results: </strong>Nirmatrelvir/ritonavir was associated with an ICER of € 395 in the immunocompromised group (per patient: + 0.125 QALYs gained; + 0.130 life-years [LYs] gained; € 49 incremental cost), with an ICER of € 8700 in 60-plus patients with comorbidity (+ 0.054 QALYs; + 0.055 LYs; € 474 incremental cost), and with an ICER of € 13,021 among 70-plus patients (+ 0.053 QALYs; + 0.045 LYs; € 689 incremental cost). Results were most sensitive to the baseline hospitalization rates among high-risk individuals. Probabilistic sensitivity analyses indicate a high probability of being cost-effective (100, 94, 85% respectively), considering a willingness-to-pay threshold of € 20,000 per QALY.</p><p><strong>Conclusions: </strong>From a Dutch societal perspective, over a lifetime horizon, nirmatrelvir/ritonavir is cost-effective versus BSC in the three groups analysed.</p>","PeriodicalId":47054,"journal":{"name":"Cost Effectiveness and Resource Allocation","volume":"23 1","pages":"5"},"PeriodicalIF":2.5000,"publicationDate":"2025-02-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11852545/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cost Effectiveness and Resource Allocation","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12962-025-00604-0","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"HEALTH POLICY & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Nirmatrelvir/ritonavir is indicated for the treatment of COVID-19 in symptomatic adults with increased risk for severe illness, not requiring supplemental oxygen yet. From a Dutch societal perspective, a cost-utility assessment of nirmatrelvir/ritonavir versus best supportive care (BSC) was conducted in three patient groups: (a) immunocompromised patients, (b) patients aged at least 60 years with one comorbidity, (c) patients aged at least 70 years. Groups were selected considering their relevance as high-risk groups, as described in Dutch and international guidelines and recommendations.
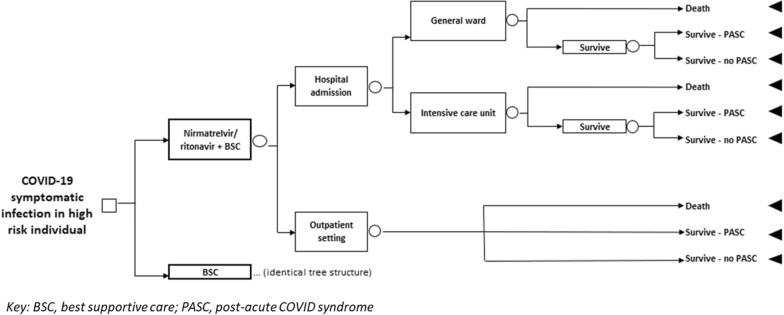
Methods: A one-year decision-tree, estimating costs and outcomes associated with a COVID-19 infection was coupled to a lifetime two-state Markov component simulating subsequent life-time survival and quality of life. Effectiveness estimates, informing the intervention preventing hospital admission or death, were based on real-world evidence by Lewnard and colleagues (2023) in a vaccinated population during a timeframe with predominance of the Omicron variant. Epidemiology relies on publicly available data, primarily sourced during the Omicron variant's era. In the decision tree, clinically relevant event-related disutilities per disease course were applied to adjusted age-dependent Dutch-specific utility levels. In the Markov component, a disutility was considered for post-ICU patients. Costs rely on Dutch pharmacoeconomic guidelines and public data sources. The incremental cost-effectiveness ratio (ICER) was analysed as the main outcome, with a positive ICER indicating the cost associated with each additional quality-adjusted life year (QALY) gained by adopting the intervention.
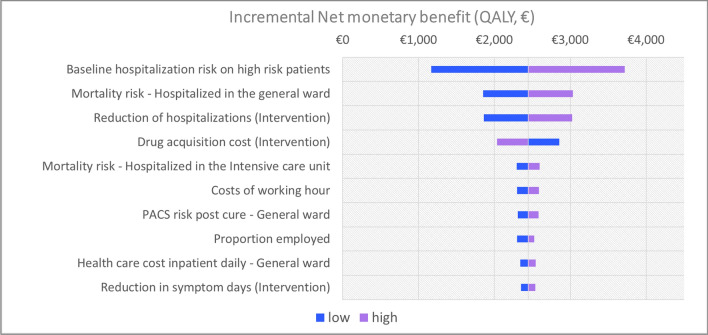
Results: Nirmatrelvir/ritonavir was associated with an ICER of € 395 in the immunocompromised group (per patient: + 0.125 QALYs gained; + 0.130 life-years [LYs] gained; € 49 incremental cost), with an ICER of € 8700 in 60-plus patients with comorbidity (+ 0.054 QALYs; + 0.055 LYs; € 474 incremental cost), and with an ICER of € 13,021 among 70-plus patients (+ 0.053 QALYs; + 0.045 LYs; € 689 incremental cost). Results were most sensitive to the baseline hospitalization rates among high-risk individuals. Probabilistic sensitivity analyses indicate a high probability of being cost-effective (100, 94, 85% respectively), considering a willingness-to-pay threshold of € 20,000 per QALY.
Conclusions: From a Dutch societal perspective, over a lifetime horizon, nirmatrelvir/ritonavir is cost-effective versus BSC in the three groups analysed.
期刊介绍:
Cost Effectiveness and Resource Allocation is an Open Access, peer-reviewed, online journal that considers manuscripts on all aspects of cost-effectiveness analysis, including conceptual or methodological work, economic evaluations, and policy analysis related to resource allocation at a national or international level. Cost Effectiveness and Resource Allocation is aimed at health economists, health services researchers, and policy-makers with an interest in enhancing the flow and transfer of knowledge relating to efficiency in the health sector. Manuscripts are encouraged from researchers based in low- and middle-income countries, with a view to increasing the international economic evidence base for health.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
