{"title":"Paternal age and neonatal outcomes: a population-based cohort study.","authors":"Wenxue Xiong, Xijia Tang, Lu Han, Li Ling","doi":"10.1093/hropen/hoaf006","DOIUrl":null,"url":null,"abstract":"<p><strong>Study question: </strong>Is paternal age associated with neonatal outcomes?</p><p><strong>Summary answer: </strong>Paternal age is independently associated with preterm birth (PTB) and caesarean section.</p><p><strong>What is known already: </strong>Advanced maternal age has long been recognized as a major risk factor for adverse neonatal outcomes. However, the association between paternal age and neonatal outcomes are not well established, yet it is biologically plausible that an increasing number of genetic and epigenetic sperm abnormalities in older males may contribute to adverse neonatal outcomes.</p><p><strong>Study design size duration: </strong>This population-based cohort study was based on the National Free Preconception Checkups Project between 1 January 2014 and 31 December 2019 in Guangdong Province, China. Paternal age at the maternal last menstrual period was measured. The main outcomes included caesarean section, PTB, small for gestational age (SGA) and perinatal infant death (PID).</p><p><strong>Participants/materials setting methods: </strong>A total of 783 988 mother-neonate-father trios were included in this study. A modified Poisson regression model was employed to estimate relative risk (RR) and 95% CI and logistic regression models were used to analyse the relative importance of predictors. We used restricted cubic splines to flexibly model the non-linear dose-response association between paternal age and neonatal outcomes. We also assessed additive interactions between paternal and maternal age on neonatal outcomes.</p><p><strong>Main results and the role of chance: </strong>Neonates born to fathers aged 35-44 years had higher risks of caesarean section (RR: 1.07; 95% CI: 1.06-1.09) and PTB (RR: 1.15; 95% CI: 1.10-1.19) compared with neonates of fathers aged 25-34 years, after adjustment for confounders. The increased risks of PTB associated with paternal age appeared to be 'dose' dependent, with a J-shaped association curve (<i>P</i> for non-linearity<0.001). The relative importance of paternal age in predicting PTB and caesarean section was similar to, or even higher than, that of maternal age. The combined effects of advanced maternal and paternal age appeared to be less than additive joint effects (relative excess risk due to interaction<0). The association of paternal age with SGA or PID was not statistically significant (<i>P </i>><i> </i>0.05).</p><p><strong>Limitations reasons for caution: </strong>As with all observational studies, residual confounding could not be ruled out. Only couples who planned to conceive were included.</p><p><strong>Wider implications of the findings: </strong>In this population-based cohort study, paternal age was independently associated with caesarean section and PTB. These findings may be clinically useful in preconception counselling on parental age-related pregnancy risks. Our findings emphasize the need to further investigate the public health implications of increasing paternal age.</p><p><strong>Study funding/competing interests: </strong>This study was supported by the Guangdong Province Medical Research Funding (No. B2023416). No competing interests are reported.</p><p><strong>Trial registration number: </strong>N/A.</p>","PeriodicalId":73264,"journal":{"name":"Human reproduction open","volume":"2025 1","pages":"hoaf006"},"PeriodicalIF":11.1000,"publicationDate":"2025-02-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11878789/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Human reproduction open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/hropen/hoaf006","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Study question: Is paternal age associated with neonatal outcomes?
Summary answer: Paternal age is independently associated with preterm birth (PTB) and caesarean section.
What is known already: Advanced maternal age has long been recognized as a major risk factor for adverse neonatal outcomes. However, the association between paternal age and neonatal outcomes are not well established, yet it is biologically plausible that an increasing number of genetic and epigenetic sperm abnormalities in older males may contribute to adverse neonatal outcomes.
Study design size duration: This population-based cohort study was based on the National Free Preconception Checkups Project between 1 January 2014 and 31 December 2019 in Guangdong Province, China. Paternal age at the maternal last menstrual period was measured. The main outcomes included caesarean section, PTB, small for gestational age (SGA) and perinatal infant death (PID).
Participants/materials setting methods: A total of 783 988 mother-neonate-father trios were included in this study. A modified Poisson regression model was employed to estimate relative risk (RR) and 95% CI and logistic regression models were used to analyse the relative importance of predictors. We used restricted cubic splines to flexibly model the non-linear dose-response association between paternal age and neonatal outcomes. We also assessed additive interactions between paternal and maternal age on neonatal outcomes.
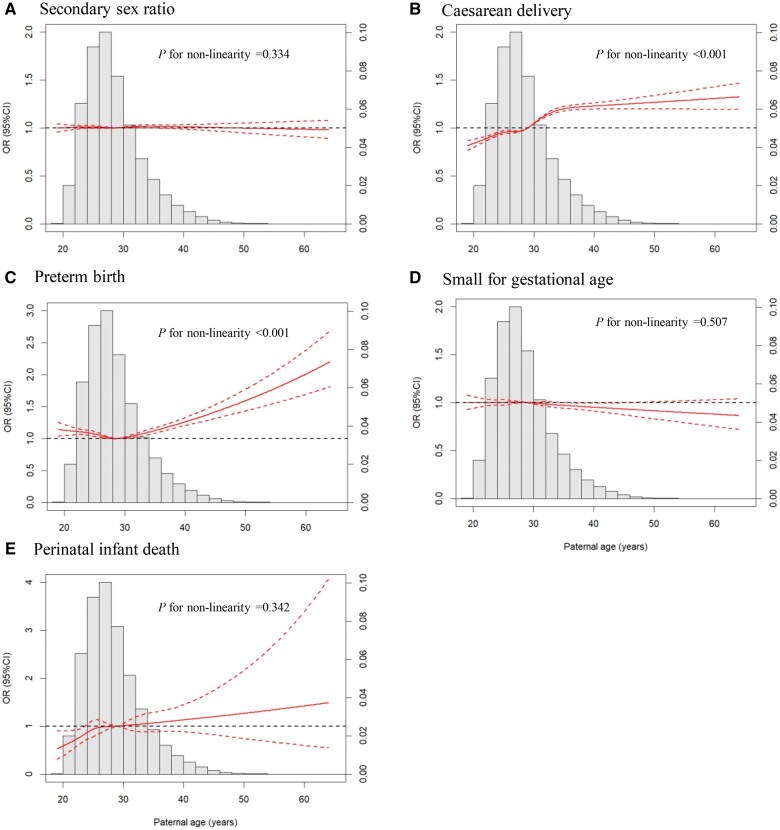
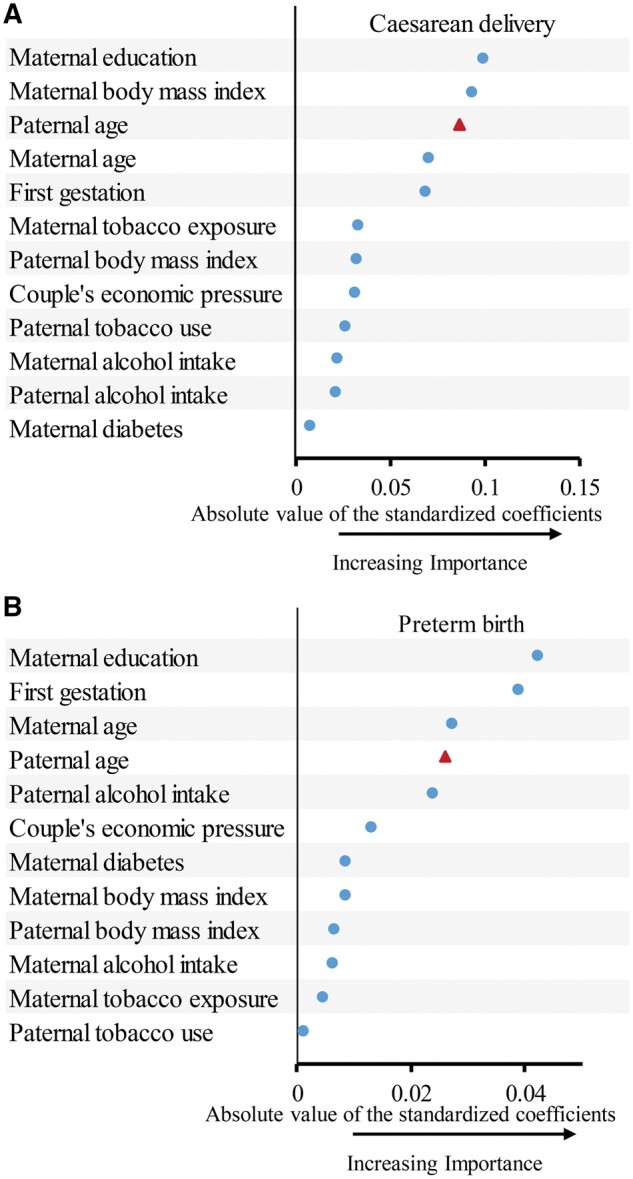
Main results and the role of chance: Neonates born to fathers aged 35-44 years had higher risks of caesarean section (RR: 1.07; 95% CI: 1.06-1.09) and PTB (RR: 1.15; 95% CI: 1.10-1.19) compared with neonates of fathers aged 25-34 years, after adjustment for confounders. The increased risks of PTB associated with paternal age appeared to be 'dose' dependent, with a J-shaped association curve (P for non-linearity<0.001). The relative importance of paternal age in predicting PTB and caesarean section was similar to, or even higher than, that of maternal age. The combined effects of advanced maternal and paternal age appeared to be less than additive joint effects (relative excess risk due to interaction<0). The association of paternal age with SGA or PID was not statistically significant (P >0.05).
Limitations reasons for caution: As with all observational studies, residual confounding could not be ruled out. Only couples who planned to conceive were included.
Wider implications of the findings: In this population-based cohort study, paternal age was independently associated with caesarean section and PTB. These findings may be clinically useful in preconception counselling on parental age-related pregnancy risks. Our findings emphasize the need to further investigate the public health implications of increasing paternal age.
Study funding/competing interests: This study was supported by the Guangdong Province Medical Research Funding (No. B2023416). No competing interests are reported.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
