Raajit K. Rampal, Sebastian Grosicki, Dominik Chraniuk, Elisabetta Abruzzese, Prithviraj Bose, Aaron T. Gerds, Alessandro M. Vannucchi, Francesca Palandri, Sung-Eun Lee, Vikas Gupta, Alessandro Lucchesi, Stephen T. Oh, Andrew T. Kuykendall, Andrea Patriarca, Alberto Álvarez-Larrán, Ruben Mesa, Jean-Jacques Kiladjian, Moshe Talpaz, Joseph M. Scandura, David Lavie, Morgan Harris, Sarah-Katharina Kays, Qing Li, Rainer Boxhammer, Barbara Brown, Anna-Maria Jegg, Claire N. Harrison, John Mascarenhas
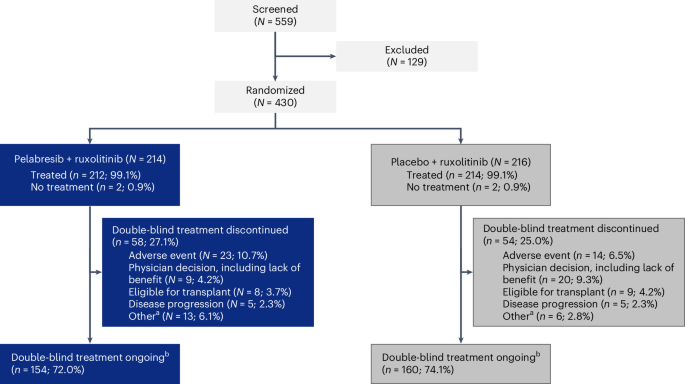
{"title":"Pelabresib plus ruxolitinib for JAK inhibitor-naive myelofibrosis: a randomized phase 3 trial","authors":"Raajit K. Rampal, Sebastian Grosicki, Dominik Chraniuk, Elisabetta Abruzzese, Prithviraj Bose, Aaron T. Gerds, Alessandro M. Vannucchi, Francesca Palandri, Sung-Eun Lee, Vikas Gupta, Alessandro Lucchesi, Stephen T. Oh, Andrew T. Kuykendall, Andrea Patriarca, Alberto Álvarez-Larrán, Ruben Mesa, Jean-Jacques Kiladjian, Moshe Talpaz, Joseph M. Scandura, David Lavie, Morgan Harris, Sarah-Katharina Kays, Qing Li, Rainer Boxhammer, Barbara Brown, Anna-Maria Jegg, Claire N. Harrison, John Mascarenhas","doi":"10.1038/s41591-025-03572-3","DOIUrl":null,"url":null,"abstract":"Janus kinase (JAK) inhibitors provide limited depth and durability of response in myelofibrosis. We evaluated pelabresib—a bromodomain and extraterminal domain (BET) inhibitor—plus ruxolitinib (a JAK inhibitor) compared with placebo plus ruxolitinib as first-line therapy. In this phase 3 study (MANIFEST-2), JAK inhibitor-naive patients with myelofibrosis were randomized 1:1 to pelabresib 125 mg once daily (QD; 50–175 mg QD permitted) for 14 days followed by a 7-day break (21-day cycle), or to placebo in combination with ruxolitinib 10 or 15 mg twice daily (BID; 5 mg QD–25 mg BID permitted). Primary endpoint was reduction in spleen volume of ≥35% from baseline at week 24. Key secondary endpoints were absolute change in total symptom score (TSS) and TSS50 response (≥50% reduction in TSS from baseline at week 24). The primary endpoint was met in 65.9% of patients randomized to pelabresib–ruxolitinib (n = 214) versus 35.2% to placebo–ruxolitinib (n = 216) (difference, 30.4%; 95% confidence interval (CI), 21.6, 39.3; P < 0.001). Absolute change in TSS was −15.99 versus −14.05 (difference, −1.94; 95% CI, −3.92, 0.04; P = 0.0545) and TSS50 was achieved in 52.3% versus 46.3% (difference, 6.0%; 95 CI, −3.5, 15.5) with pelabresib–ruxolitinib versus placebo–ruxolitinib. Exploratory analyses of proinflammatory cytokine amounts and bone marrow morphology showed greater improvement with the combination. Thrombocytopenia and anemia were the most common treatment-emergent adverse events, occurring in 52.8% (13.2% grade ≥3) versus 37.4% (6.1% grade ≥3) and 44.8% (23.1% grade ≥3) versus 55.1% (36.5% grade ≥3), respectively. Pelabresib in combination with ruxolitinib is well tolerated, improves signs of underlying myelofibrosis pathobiology and provides substantial clinical benefit over standard-of-care JAK inhibitor monotherapy. ClinicalTrials.gov identifier: NCT04603495 . In a randomized phase 3 trial, the combination of the BET inhibitor pelabresib with the JAK inhibitor ruxolitinib resulted in a significantly higher spleen volume reduction from baseline versus placebo with ruxolitinib in patients with JAK inhibitor-naive myelofibrosis.","PeriodicalId":19037,"journal":{"name":"Nature Medicine","volume":"31 5","pages":"1531-1538"},"PeriodicalIF":50.0000,"publicationDate":"2025-03-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.nature.comhttps://www.nature.com/articles/s41591-025-03572-3.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Nature Medicine","FirstCategoryId":"3","ListUrlMain":"https://www.nature.com/articles/s41591-025-03572-3","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"BIOCHEMISTRY & MOLECULAR BIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Janus kinase (JAK) inhibitors provide limited depth and durability of response in myelofibrosis. We evaluated pelabresib—a bromodomain and extraterminal domain (BET) inhibitor—plus ruxolitinib (a JAK inhibitor) compared with placebo plus ruxolitinib as first-line therapy. In this phase 3 study (MANIFEST-2), JAK inhibitor-naive patients with myelofibrosis were randomized 1:1 to pelabresib 125 mg once daily (QD; 50–175 mg QD permitted) for 14 days followed by a 7-day break (21-day cycle), or to placebo in combination with ruxolitinib 10 or 15 mg twice daily (BID; 5 mg QD–25 mg BID permitted). Primary endpoint was reduction in spleen volume of ≥35% from baseline at week 24. Key secondary endpoints were absolute change in total symptom score (TSS) and TSS50 response (≥50% reduction in TSS from baseline at week 24). The primary endpoint was met in 65.9% of patients randomized to pelabresib–ruxolitinib (n = 214) versus 35.2% to placebo–ruxolitinib (n = 216) (difference, 30.4%; 95% confidence interval (CI), 21.6, 39.3; P < 0.001). Absolute change in TSS was −15.99 versus −14.05 (difference, −1.94; 95% CI, −3.92, 0.04; P = 0.0545) and TSS50 was achieved in 52.3% versus 46.3% (difference, 6.0%; 95 CI, −3.5, 15.5) with pelabresib–ruxolitinib versus placebo–ruxolitinib. Exploratory analyses of proinflammatory cytokine amounts and bone marrow morphology showed greater improvement with the combination. Thrombocytopenia and anemia were the most common treatment-emergent adverse events, occurring in 52.8% (13.2% grade ≥3) versus 37.4% (6.1% grade ≥3) and 44.8% (23.1% grade ≥3) versus 55.1% (36.5% grade ≥3), respectively. Pelabresib in combination with ruxolitinib is well tolerated, improves signs of underlying myelofibrosis pathobiology and provides substantial clinical benefit over standard-of-care JAK inhibitor monotherapy. ClinicalTrials.gov identifier: NCT04603495 . In a randomized phase 3 trial, the combination of the BET inhibitor pelabresib with the JAK inhibitor ruxolitinib resulted in a significantly higher spleen volume reduction from baseline versus placebo with ruxolitinib in patients with JAK inhibitor-naive myelofibrosis.
期刊介绍:
Nature Medicine is a monthly journal publishing original peer-reviewed research in all areas of medicine. The publication focuses on originality, timeliness, interdisciplinary interest, and the impact on improving human health. In addition to research articles, Nature Medicine also publishes commissioned content such as News, Reviews, and Perspectives. This content aims to provide context for the latest advances in translational and clinical research, reaching a wide audience of M.D. and Ph.D. readers. All editorial decisions for the journal are made by a team of full-time professional editors.
Nature Medicine consider all types of clinical research, including:
-Case-reports and small case series
-Clinical trials, whether phase 1, 2, 3 or 4
-Observational studies
-Meta-analyses
-Biomarker studies
-Public and global health studies
Nature Medicine is also committed to facilitating communication between translational and clinical researchers. As such, we consider “hybrid” studies with preclinical and translational findings reported alongside data from clinical studies.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
