{"title":"A Nomogram for Predicting Survival in Patients with Respiratory Failure Following Trauma: A Retrospective Study Using the MIMIC-IV Database.","authors":"Peihan Li, Xuejuan Wang, Li Li","doi":"10.2147/DHPS.S497413","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Respiratory failure (RF) after trauma is one of the major causes of patients being admitted to the ICU and leads to a high mortality rate. However, we cannot predict mortality rates based on patients' various indicators. The aim of this study is to develop and validate a nomogram for predicting mortality in patients in the intensive care unit (ICU).</p><p><strong>Methods: </strong>A total of 377 patients from the Medical Information Mart for Intensive Care (MIMIC)-IV database were included in the study. All participants were systematically divided into a development cohort for modelling and a validation cohort for internal validation at a ratio of 7:3. Following patient admission, a comprehensive collection of 30 clinical indicators was performed. The least absolute shrinkage and selection operator (LASSO) regression technique was employed to discern pivotal risk factors. A multivariate Cox regression model was established, and a receiver operating curve (ROC) was plotted, and the area under the curve (AUC) was calculated. Furthermore, the decision curve analysis (DCA) was performed, and the nomogram was compared with the acute physiology score III (APSIII) and Oxford acute severity of illness score (OASIS) scoring systems to assess the net clinical benefit.</p><p><strong>Results: </strong>The indicators included in our model were age, OASIS score, SAPS III score, respiratory rate (RR), blood urea nitrogen (BUN) and hematocrit. The results demonstrated that our model yielded satisfied performance on the development cohort and on internal validation. The calibration curve underscored a robust concordance between predicted and actual outcomes. The DCA showed a superior clinical utility of our model in contrast to previously reported scoring systems.</p><p><strong>Conclusion: </strong>In summary, we devised a nomogram for predicting mortality during the ICU stay of RF patients following trauma and established a prediction model that facilitates clinical decision making. However, external validation is needed in the future.</p>","PeriodicalId":11377,"journal":{"name":"Drug, Healthcare and Patient Safety","volume":"17 ","pages":"63-74"},"PeriodicalIF":3.4000,"publicationDate":"2025-03-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11890444/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Drug, Healthcare and Patient Safety","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/DHPS.S497413","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Respiratory failure (RF) after trauma is one of the major causes of patients being admitted to the ICU and leads to a high mortality rate. However, we cannot predict mortality rates based on patients' various indicators. The aim of this study is to develop and validate a nomogram for predicting mortality in patients in the intensive care unit (ICU).
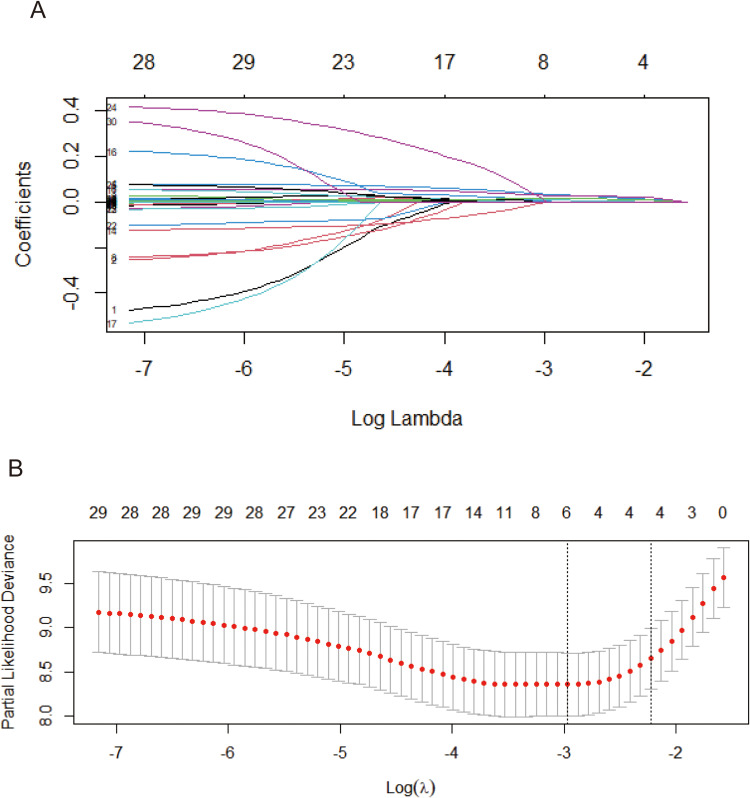
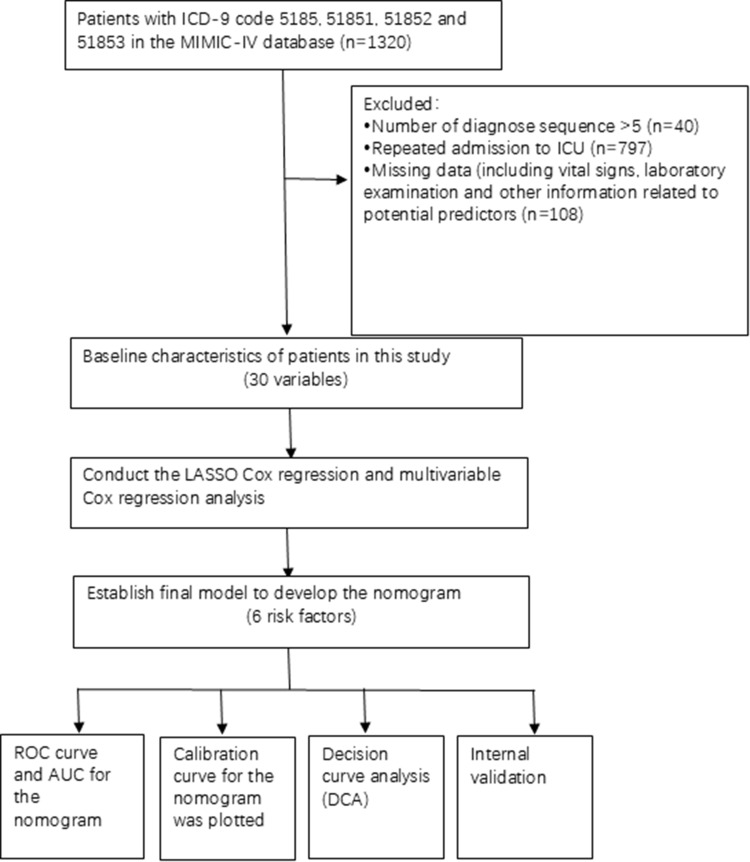
Methods: A total of 377 patients from the Medical Information Mart for Intensive Care (MIMIC)-IV database were included in the study. All participants were systematically divided into a development cohort for modelling and a validation cohort for internal validation at a ratio of 7:3. Following patient admission, a comprehensive collection of 30 clinical indicators was performed. The least absolute shrinkage and selection operator (LASSO) regression technique was employed to discern pivotal risk factors. A multivariate Cox regression model was established, and a receiver operating curve (ROC) was plotted, and the area under the curve (AUC) was calculated. Furthermore, the decision curve analysis (DCA) was performed, and the nomogram was compared with the acute physiology score III (APSIII) and Oxford acute severity of illness score (OASIS) scoring systems to assess the net clinical benefit.
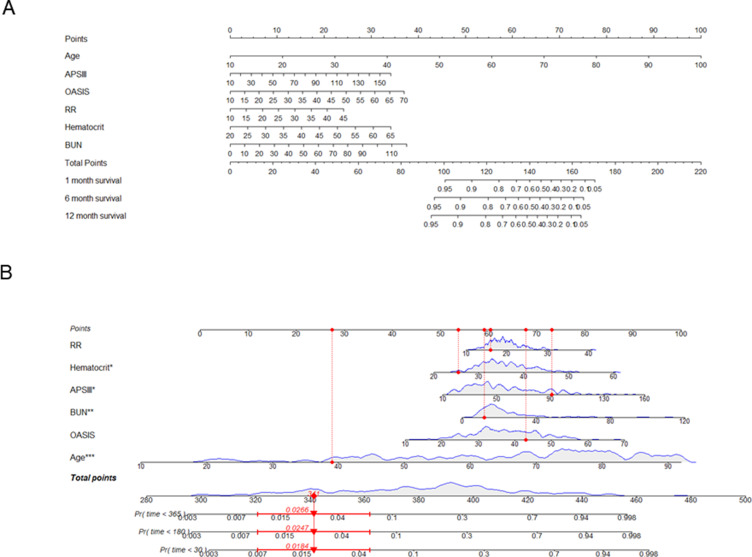
Results: The indicators included in our model were age, OASIS score, SAPS III score, respiratory rate (RR), blood urea nitrogen (BUN) and hematocrit. The results demonstrated that our model yielded satisfied performance on the development cohort and on internal validation. The calibration curve underscored a robust concordance between predicted and actual outcomes. The DCA showed a superior clinical utility of our model in contrast to previously reported scoring systems.
Conclusion: In summary, we devised a nomogram for predicting mortality during the ICU stay of RF patients following trauma and established a prediction model that facilitates clinical decision making. However, external validation is needed in the future.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
