Mohammed A Almeshari, Nowaf Y Alobaidi, James A Stockley, Robert A Stockley, Prasad Nagakumar, Benjamin Paul Sutton, Elizabeth Sapey
{"title":"Physiological Small Airways Dysfunction and the Bronchodilator Response in Adults With Asthma and Its Risk Factors: A Retrospective Analysis.","authors":"Mohammed A Almeshari, Nowaf Y Alobaidi, James A Stockley, Robert A Stockley, Prasad Nagakumar, Benjamin Paul Sutton, Elizabeth Sapey","doi":"10.2147/JAA.S489893","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Physiological evidence of small airways dysfunction (SAD) is present in some patients with asthma and is associated with poor disease control. It is unclear if this represents a distinct phenotype of asthma or if it is an early manifestation of the disease. The study aimed to evaluate SAD in asthma and its clinical associations.</p><p><strong>Methods: </strong>A retrospective analysis of routinely collected health data obtained from adults referred for routine spirometric assessment as part of their clinical management. The Maximal Mid-Expiratory Flow (MMEF) z-scores were used to assess the prevalence and association factors for SAD. Pre- and post-bronchodilator data of MMEF and FEV<sub>1</sub> in patients with and without SAD or airflow obstruction (AO) were analysed.</p><p><strong>Results: </strong>A total of 1094 patients were included. 366 (33.5%) had evidence of SAD of whom 261 (71.3%) also had AO. Current smokers were at an increased risk of having SAD (OR: 2.05; 95% CI: 1.43-2.93). 214 patients had Bronchodilator response (BDR) data with 157 (73.4%) demonstrating BDR for MMEF and 121 (56.5%) for FEV<sub>1</sub>. SAD at baseline was associated with a significant BDR for FEV<sub>1</sub> (OR of 3.59 (95% CI: 1.77-7.57)) and MMEF (OR of 2.89 (95% CI: 1.41-5.95)). Males were less likely to have a positive BDR for MMEF than females (OR of 0.46; 95% CI: 0.24-0.89).</p><p><strong>Conclusion: </strong>SAD is common in asthma and is related to the presence of AO, cigarette smoking and is associated with increased BDR for both FEV<sub>1</sub> and MMEF. The assessment of SAD in routine clinical practice may help identify airway impairment early for the initiation of targeted therapies.</p>","PeriodicalId":15079,"journal":{"name":"Journal of Asthma and Allergy","volume":"18 ","pages":"377-389"},"PeriodicalIF":3.0000,"publicationDate":"2025-03-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11892509/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Asthma and Allergy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2147/JAA.S489893","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ALLERGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Physiological evidence of small airways dysfunction (SAD) is present in some patients with asthma and is associated with poor disease control. It is unclear if this represents a distinct phenotype of asthma or if it is an early manifestation of the disease. The study aimed to evaluate SAD in asthma and its clinical associations.
Methods: A retrospective analysis of routinely collected health data obtained from adults referred for routine spirometric assessment as part of their clinical management. The Maximal Mid-Expiratory Flow (MMEF) z-scores were used to assess the prevalence and association factors for SAD. Pre- and post-bronchodilator data of MMEF and FEV1 in patients with and without SAD or airflow obstruction (AO) were analysed.
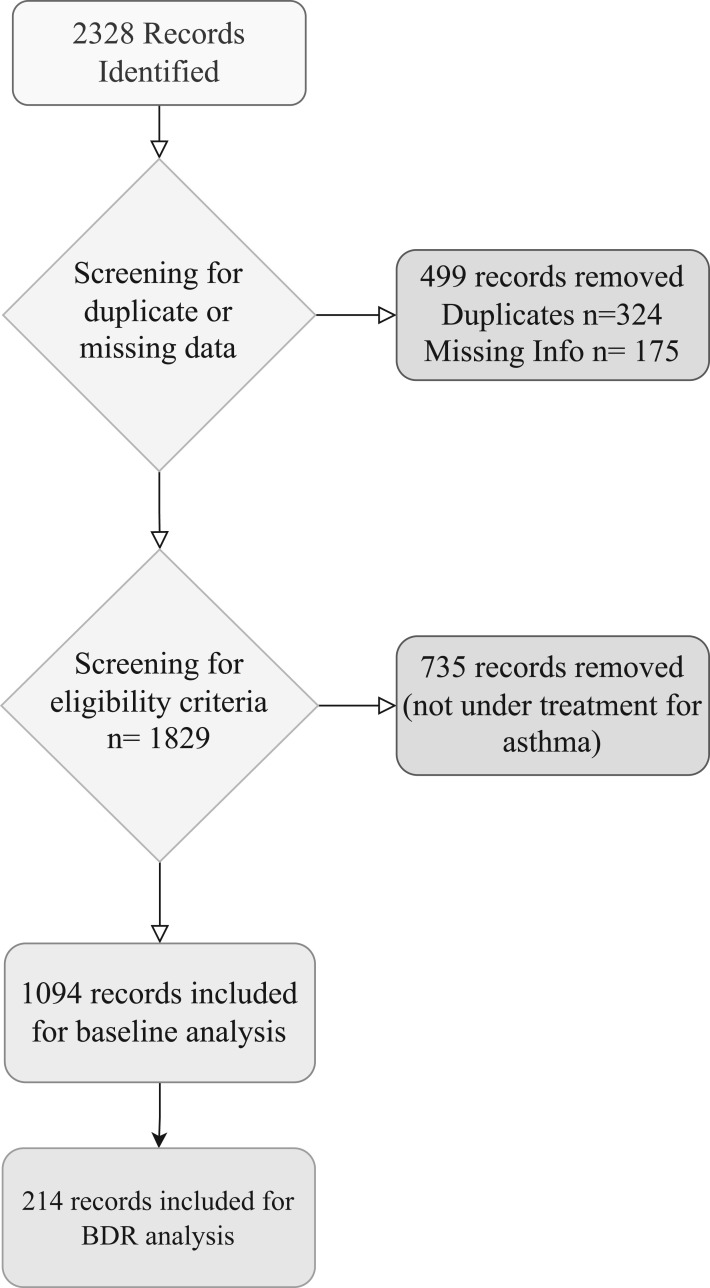
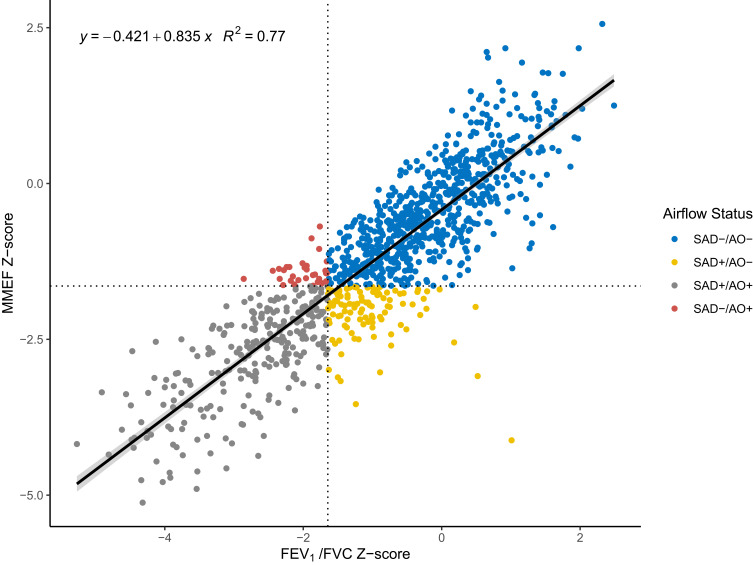
Results: A total of 1094 patients were included. 366 (33.5%) had evidence of SAD of whom 261 (71.3%) also had AO. Current smokers were at an increased risk of having SAD (OR: 2.05; 95% CI: 1.43-2.93). 214 patients had Bronchodilator response (BDR) data with 157 (73.4%) demonstrating BDR for MMEF and 121 (56.5%) for FEV1. SAD at baseline was associated with a significant BDR for FEV1 (OR of 3.59 (95% CI: 1.77-7.57)) and MMEF (OR of 2.89 (95% CI: 1.41-5.95)). Males were less likely to have a positive BDR for MMEF than females (OR of 0.46; 95% CI: 0.24-0.89).
Conclusion: SAD is common in asthma and is related to the presence of AO, cigarette smoking and is associated with increased BDR for both FEV1 and MMEF. The assessment of SAD in routine clinical practice may help identify airway impairment early for the initiation of targeted therapies.
期刊介绍:
An international, peer-reviewed journal publishing original research, reports, editorials and commentaries on the following topics: Asthma; Pulmonary physiology; Asthma related clinical health; Clinical immunology and the immunological basis of disease; Pharmacological interventions and new therapies.
Although the main focus of the journal will be to publish research and clinical results in humans, preclinical, animal and in vitro studies will be published where they shed light on disease processes and potential new therapies.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
