Extended pharmacological thromboprophylaxis and clinically relevant venous thromboembolism after major abdominal and pelvic surgery: international, prospective, propensity score-weighted cohort study.
{"title":"Extended pharmacological thromboprophylaxis and clinically relevant venous thromboembolism after major abdominal and pelvic surgery: international, prospective, propensity score-weighted cohort study.","authors":"","doi":"10.1093/bjs/znaf005","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>There is low-certainty evidence on the impact of extended pharmacological prophylaxis on venous thromboembolism-associated morbidity and mortality. The aim of this study was to determine the efficacy and safety of extended prophylaxis after major abdominopelvic surgery for the prevention of clinically relevant venous thromboembolism after hospital discharge.</p><p><strong>Methods: </strong>CArdiovaSCulAr outcomes after major abDominal surgEry (CASCADE) was a prospective, international, cohort study into which consecutive adult patients undergoing major abdominopelvic surgery were enrolled (January-May 2022). Extended prophylaxis was considered at least 28 days of anticoagulant prescription after surgery. The primary efficacy outcome was clinically relevant venous thromboembolism and the primary safety outcome was clinically relevant bleeding within 30 days after surgery (European Medicines Agency definitions). The independent association of these outcomes with extended prophylaxis was explored using mixed-effects logistic regression and propensity score weighting.</p><p><strong>Results: </strong>A total of 11 571 patients (median age of 58.0 years; 6399 (55.3%) women) from 29 countries were included. The extended prophylaxis prescription rate was 31.7% (3670 patients). The post-discharge venous thromboembolism and bleeding rates were 0.1% (12 patients) and 0.7% (85 patients) respectively. After weighting, extended prophylaxis was not significantly associated with increased bleeding risk (OR 1.07 (95% c.i. 0.64 to 1.81); P = 0.792) or decreased venous thromboembolism incidence, both in the overall cohort (OR 1.13 (95% c.i. 0.33 to 3.90); P = 0.848) and in a subgroup analysis of patients undergoing complex major surgery and with active cancer (OR: 1.36 (95% c.i. 0.33 to 5.57); P = 0.669).</p><p><strong>Conclusion: </strong>In modern practice, the incidence of postoperative venous thromboembolism is low. Extended prophylaxis appears safe, yet the clinical efficacy remains uncertain. Further work is required to define patients who stand to benefit.</p>","PeriodicalId":136,"journal":{"name":"British Journal of Surgery","volume":"112 3","pages":""},"PeriodicalIF":8.8000,"publicationDate":"2025-03-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11894929/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"British Journal of Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/bjs/znaf005","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: There is low-certainty evidence on the impact of extended pharmacological prophylaxis on venous thromboembolism-associated morbidity and mortality. The aim of this study was to determine the efficacy and safety of extended prophylaxis after major abdominopelvic surgery for the prevention of clinically relevant venous thromboembolism after hospital discharge.
Methods: CArdiovaSCulAr outcomes after major abDominal surgEry (CASCADE) was a prospective, international, cohort study into which consecutive adult patients undergoing major abdominopelvic surgery were enrolled (January-May 2022). Extended prophylaxis was considered at least 28 days of anticoagulant prescription after surgery. The primary efficacy outcome was clinically relevant venous thromboembolism and the primary safety outcome was clinically relevant bleeding within 30 days after surgery (European Medicines Agency definitions). The independent association of these outcomes with extended prophylaxis was explored using mixed-effects logistic regression and propensity score weighting.
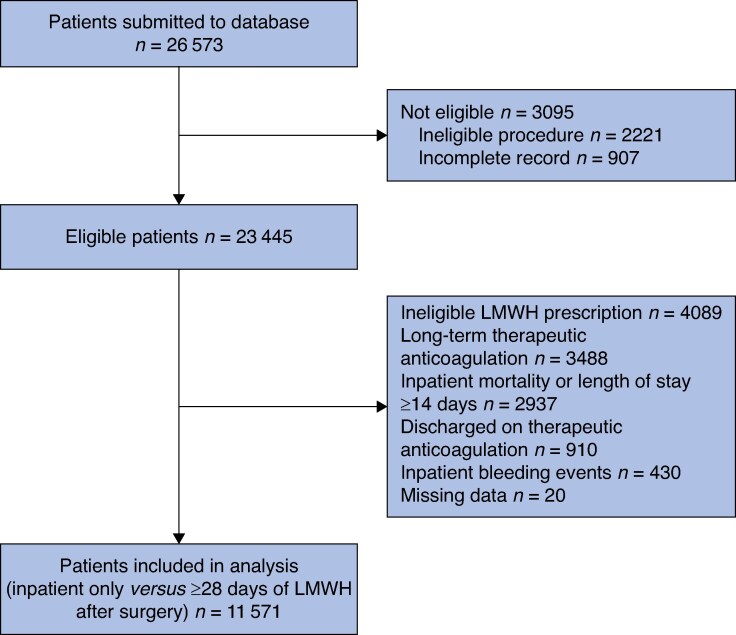
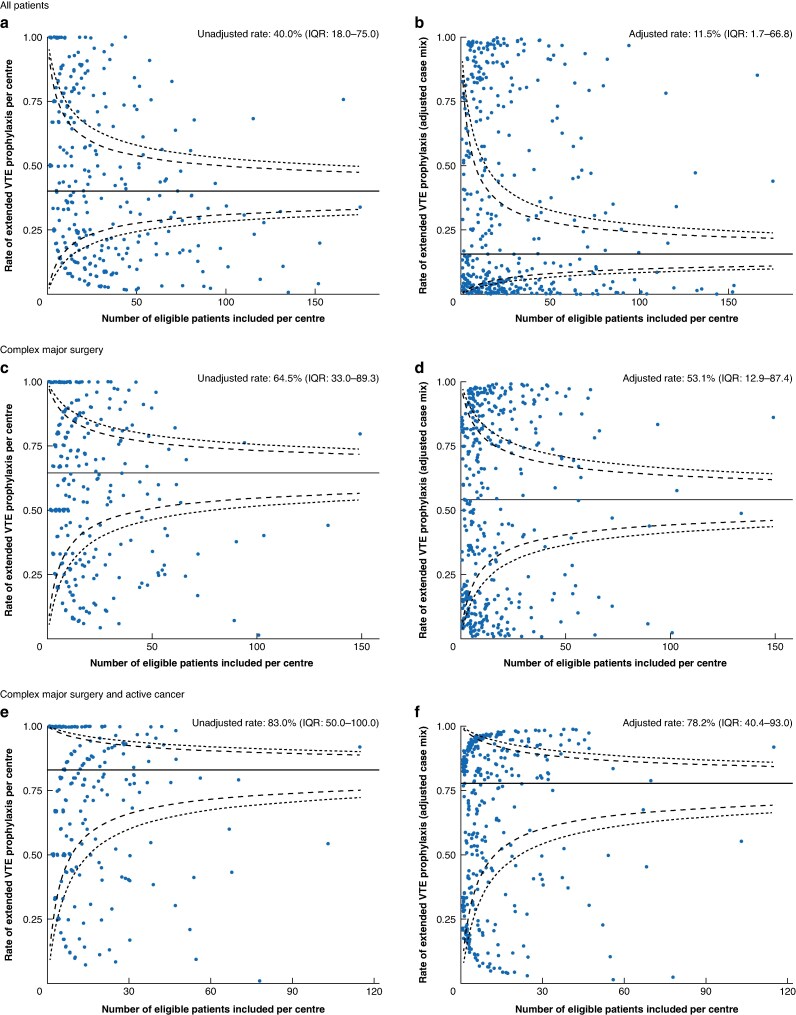
Results: A total of 11 571 patients (median age of 58.0 years; 6399 (55.3%) women) from 29 countries were included. The extended prophylaxis prescription rate was 31.7% (3670 patients). The post-discharge venous thromboembolism and bleeding rates were 0.1% (12 patients) and 0.7% (85 patients) respectively. After weighting, extended prophylaxis was not significantly associated with increased bleeding risk (OR 1.07 (95% c.i. 0.64 to 1.81); P = 0.792) or decreased venous thromboembolism incidence, both in the overall cohort (OR 1.13 (95% c.i. 0.33 to 3.90); P = 0.848) and in a subgroup analysis of patients undergoing complex major surgery and with active cancer (OR: 1.36 (95% c.i. 0.33 to 5.57); P = 0.669).
Conclusion: In modern practice, the incidence of postoperative venous thromboembolism is low. Extended prophylaxis appears safe, yet the clinical efficacy remains uncertain. Further work is required to define patients who stand to benefit.
期刊介绍:
The British Journal of Surgery (BJS), incorporating the European Journal of Surgery, stands as Europe's leading peer-reviewed surgical journal. It serves as an invaluable platform for presenting high-quality clinical and laboratory-based research across a wide range of surgical topics. In addition to providing a comprehensive coverage of traditional surgical practices, BJS also showcases emerging areas in the field, such as minimally invasive therapy and interventional radiology.
While the journal appeals to general surgeons, it also holds relevance for specialty surgeons and professionals working in closely related fields. By presenting cutting-edge research and advancements, BJS aims to revolutionize the way surgical knowledge is shared and contribute to the ongoing progress of the surgical community.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
