Matthew Spotnitz, John Giannini, Yechiam Ostchega, Stephanie L Goff, Lakshmi Priya Anandan, Emily Clark, Tamara R Litwin, Lew Berman
{"title":"Assessing the Data Quality Dimensions of Partial and Complete Mastectomy Cohorts in the <i>All of Us</i> Research Program: Cross-Sectional Study.","authors":"Matthew Spotnitz, John Giannini, Yechiam Ostchega, Stephanie L Goff, Lakshmi Priya Anandan, Emily Clark, Tamara R Litwin, Lew Berman","doi":"10.2196/59298","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Breast cancer is prevalent among females in the United States. Nonmetastatic disease is treated by partial or complete mastectomy procedures. However, the rates of those procedures vary across practices. Generating real-world evidence on breast cancer surgery could lead to improved and consistent practices. We investigated the quality of data from the All of Us Research Program, which is a precision medicine initiative that collected real-world electronic health care data from different sites in the United States both retrospectively and prospectively to participant enrollment.</p><p><strong>Objective: </strong>The paper aims to determine whether All of Us data are fit for use in generating real-world evidence on mastectomy procedures.</p><p><strong>Methods: </strong>Our mastectomy phenotype consisted of adult female participants who had CPT4 (Current Procedural Terminology 4), ICD-9 (International Classification of Diseases, Ninth Revision) procedure, or SNOMED (Systematized Nomenclature of Medicine) codes for a partial or complete mastectomy procedure that mapped to Observational Medical Outcomes Partnership Common Data Model concepts. We evaluated the phenotype with a data quality dimensions (DQD) framework that consisted of 5 elements: conformance, completeness, concordance, plausibility, and temporality. Also, we applied a previously developed DQD checklist to evaluate concept selection, internal verification, and external validation for each dimension. We compared the DQD of our cohort to a control group of adult women who did not have a mastectomy procedure. Our subgroup analysis compared partial to complete mastectomy procedure phenotypes.</p><p><strong>Results: </strong>There were 4175 female participants aged 18 years or older in the partial or complete mastectomy cohort, and 168,226 participants in the control cohort. The geospatial distribution of our cohort varied across states. For example, our cohort consisted of 835 (20%) participants from Massachusetts, but multiple other states contributed fewer than 20 participants. We compared the sociodemographic characteristics of the partial (n=2607) and complete (n=1568) mastectomy subgroups. Those groups differed in the distribution of age at procedure (P<.001), education (P=.02), and income (P=.03) levels, as per χ2 analysis. A total of 367 (9.9%) participants in our cohort had overlapping CPT4 and SNOMED codes for a mastectomy, and 63 (1.5%) had overlapping ICD-9 procedure and SNOMED codes. The prevalence of breast cancer-related concepts was higher in our cohort compared to the control group (P<.001). In both the partial and complete mastectomy subgroups, the correlations among concepts were consistent with the clinical management of breast cancer. The median time between biopsy and mastectomy was 5.5 (IQR 3.5-11.2) weeks. Although we did not have external benchmark comparisons, we were able to evaluate concept selection and internal verification for all domains.</p><p><strong>Conclusions: </strong>Our data quality framework was implemented successfully on a mastectomy phenotype. Our systematic approach identified data missingness. Moreover, the framework allowed us to differentiate breast-conserving therapy and complete mastectomy subgroups in the All of Us data.</p>","PeriodicalId":45538,"journal":{"name":"JMIR Cancer","volume":"11 ","pages":"e59298"},"PeriodicalIF":2.7000,"publicationDate":"2025-03-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11918980/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JMIR Cancer","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2196/59298","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Breast cancer is prevalent among females in the United States. Nonmetastatic disease is treated by partial or complete mastectomy procedures. However, the rates of those procedures vary across practices. Generating real-world evidence on breast cancer surgery could lead to improved and consistent practices. We investigated the quality of data from the All of Us Research Program, which is a precision medicine initiative that collected real-world electronic health care data from different sites in the United States both retrospectively and prospectively to participant enrollment.
Objective: The paper aims to determine whether All of Us data are fit for use in generating real-world evidence on mastectomy procedures.
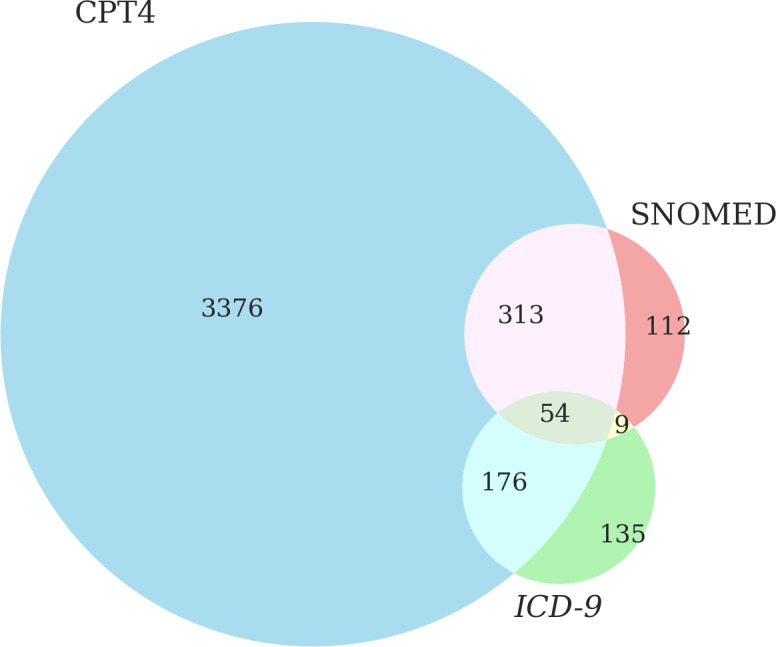
Methods: Our mastectomy phenotype consisted of adult female participants who had CPT4 (Current Procedural Terminology 4), ICD-9 (International Classification of Diseases, Ninth Revision) procedure, or SNOMED (Systematized Nomenclature of Medicine) codes for a partial or complete mastectomy procedure that mapped to Observational Medical Outcomes Partnership Common Data Model concepts. We evaluated the phenotype with a data quality dimensions (DQD) framework that consisted of 5 elements: conformance, completeness, concordance, plausibility, and temporality. Also, we applied a previously developed DQD checklist to evaluate concept selection, internal verification, and external validation for each dimension. We compared the DQD of our cohort to a control group of adult women who did not have a mastectomy procedure. Our subgroup analysis compared partial to complete mastectomy procedure phenotypes.
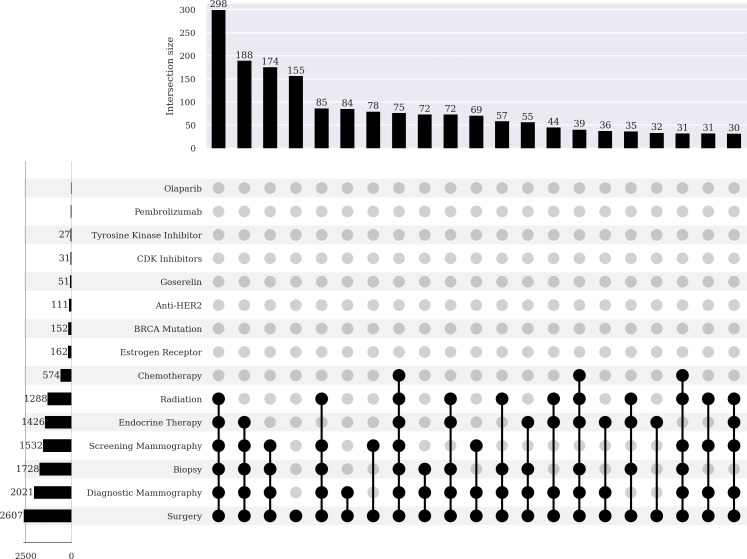
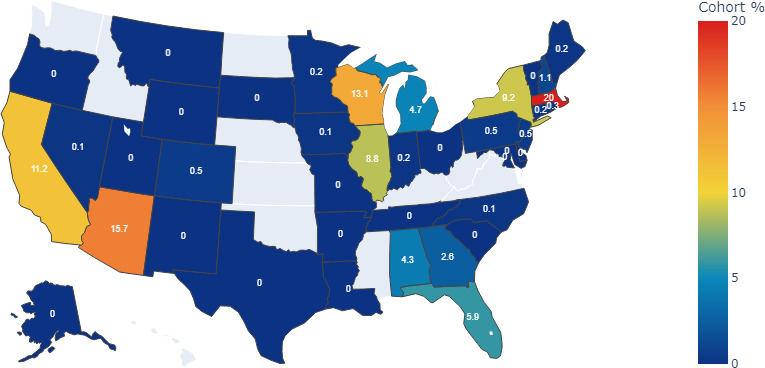
Results: There were 4175 female participants aged 18 years or older in the partial or complete mastectomy cohort, and 168,226 participants in the control cohort. The geospatial distribution of our cohort varied across states. For example, our cohort consisted of 835 (20%) participants from Massachusetts, but multiple other states contributed fewer than 20 participants. We compared the sociodemographic characteristics of the partial (n=2607) and complete (n=1568) mastectomy subgroups. Those groups differed in the distribution of age at procedure (P<.001), education (P=.02), and income (P=.03) levels, as per χ2 analysis. A total of 367 (9.9%) participants in our cohort had overlapping CPT4 and SNOMED codes for a mastectomy, and 63 (1.5%) had overlapping ICD-9 procedure and SNOMED codes. The prevalence of breast cancer-related concepts was higher in our cohort compared to the control group (P<.001). In both the partial and complete mastectomy subgroups, the correlations among concepts were consistent with the clinical management of breast cancer. The median time between biopsy and mastectomy was 5.5 (IQR 3.5-11.2) weeks. Although we did not have external benchmark comparisons, we were able to evaluate concept selection and internal verification for all domains.
Conclusions: Our data quality framework was implemented successfully on a mastectomy phenotype. Our systematic approach identified data missingness. Moreover, the framework allowed us to differentiate breast-conserving therapy and complete mastectomy subgroups in the All of Us data.
背景:乳腺癌在美国女性中很普遍。非转移性疾病通过部分或全部乳房切除术治疗。然而,这些程序的比率因实践而异。产生关于乳腺癌手术的真实证据可能会导致改进和一致的做法。我们调查了来自“我们所有人研究计划”的数据质量,该计划是一项精密医学倡议,收集了来自美国不同地点的真实电子医疗保健数据,包括回顾性和前瞻性的参与者登记。目的:本文旨在确定All of Us数据是否适合用于生成乳腺切除术过程的真实证据。方法:我们的乳房切除术表型包括具有CPT4(现行程序术语4),ICD-9(国际疾病分类,第九次修订)程序或SNOMED(系统化医学命名法)代码的部分或完全乳房切除术的成年女性参与者,这些代码映射到观察性医疗结果伙伴关系公共数据模型概念。我们用数据质量维度(DQD)框架评估表型,该框架由5个要素组成:一致性、完整性、一致性、合理性和时间性。此外,我们应用了先前开发的DQD检查表来评估每个维度的概念选择、内部验证和外部验证。我们将我们队列的DQD与未做过乳房切除术的成年女性的对照组进行了比较。我们的亚组分析比较了部分和完全乳房切除术的表型。结果:在乳房部分或完全切除术队列中,有4175名18岁及以上的女性参与者,对照组中有168,226名参与者。我们的队列在各州的地理空间分布各不相同。例如,我们的队列由来自马萨诸塞州的835名(20%)参与者组成,但其他多个州的参与者人数不到20人。我们比较了部分(n=2607)和完全(n=1568)乳房切除术亚组的社会人口学特征。这些组在手术年龄分布上存在差异(结论:我们的数据质量框架在乳房切除术表型上成功实施。我们的系统方法确定了数据缺失。此外,该框架允许我们在All of us数据中区分保乳治疗和完全乳房切除术亚组。



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
