{"title":"MRI and <sup>18</sup>F-FDG-PET/CT findings of cervical reactive lymphadenitis: a comparison with nodal lymphoma.","authors":"Hiroki Kato, Tomohiro Ando, Yusuke Kito, Hirofumi Shibata, Takenori Ogawa, Takuya Seko, Masaya Kawaguchi, Yoshifumi Noda, Fuminori Hyodo, Masayuki Matsuo","doi":"10.5114/pjr/196644","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>This study aimed to compare the findings of magnetic resonance imaging (MRI) and <sup>18</sup>F-fluorodeoxyglucose (FDG)-positron emission tomography/computed tomography (PET/CT) to differentiate reactive lymphadenitis from nodal lymphoma of the head and neck.</p><p><strong>Material and methods: </strong>This study included 138 patients with histopathologically confirmed cervical lymphadenopathy, including 35 patients with reactive lymphadenitis and 103 patients with nodal lymphoma, who had neck MRI (<i>n</i> = 63) and/or <sup>18</sup>F-FDG-PET/CT (<i>n</i> = 123) before biopsy. The quantitative and qualitative MRI results and maximum standardised uptake value (SUV<sub>max</sub>) were retrospectively analysed and compared between the 2 pathologies.</p><p><strong>Results: </strong>The maximum diameter (22.4 ± 6.9 vs. 33.3 ± 16.0 mm, <i>p</i> < 0.01), minimum diameter (15.8 ± 3.6 vs. 22.3 ± 8.5 mm, <i>p</i> < 0.01), and SUV<sub>max</sub> (6.9 ± 2.7 vs. 12.8 ± 8.0, <i>p</i> < 0.01) of the lesion were lower in reactive lymphadenitis than in nodal lymphoma, respectively. T2-hypointense-thickened capsules > 2 mm (46% vs. 14%, <i>p</i> < 0.05) and T2-hypointense areas converging to the periphery (15% vs. 0%, <i>p</i> < 0.05) were more frequently observed in reactive lymphadenitis than in nodal lymphoma, respectively. Hilum of nodes on T2-weighted images (54% vs. 22%, <i>p</i> < 0.05) and diffusion-weighted images (69% vs. 30%, <i>p</i> < 0.05) were more frequently demonstrated in reactive lymphadenitis than in nodal lymphoma, respectively.</p><p><strong>Conclusions: </strong>Reactive lymphadenitis had a smaller size and lower SUV<sub>max</sub>. The presence of T2-hypointense-thickened capsules, T2-hypointense areas converging to the periphery, and hilum of nodes were signs of reactive lymphadenitis.</p>","PeriodicalId":94174,"journal":{"name":"Polish journal of radiology","volume":"90 ","pages":"e9-e18"},"PeriodicalIF":0.0000,"publicationDate":"2025-01-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11891550/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Polish journal of radiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5114/pjr/196644","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: This study aimed to compare the findings of magnetic resonance imaging (MRI) and 18F-fluorodeoxyglucose (FDG)-positron emission tomography/computed tomography (PET/CT) to differentiate reactive lymphadenitis from nodal lymphoma of the head and neck.
Material and methods: This study included 138 patients with histopathologically confirmed cervical lymphadenopathy, including 35 patients with reactive lymphadenitis and 103 patients with nodal lymphoma, who had neck MRI (n = 63) and/or 18F-FDG-PET/CT (n = 123) before biopsy. The quantitative and qualitative MRI results and maximum standardised uptake value (SUVmax) were retrospectively analysed and compared between the 2 pathologies.
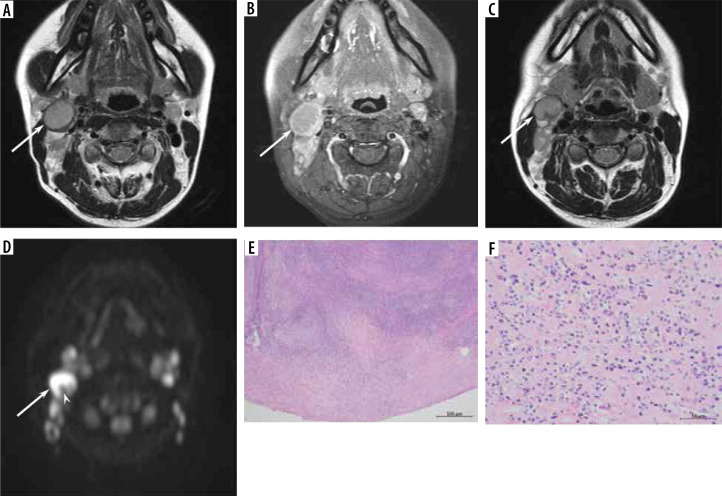
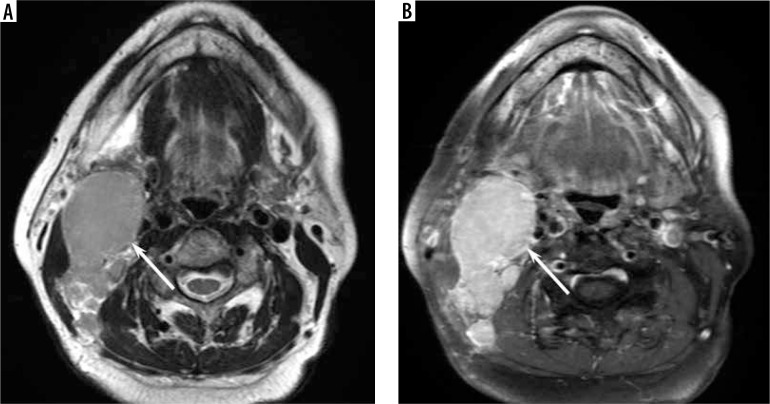
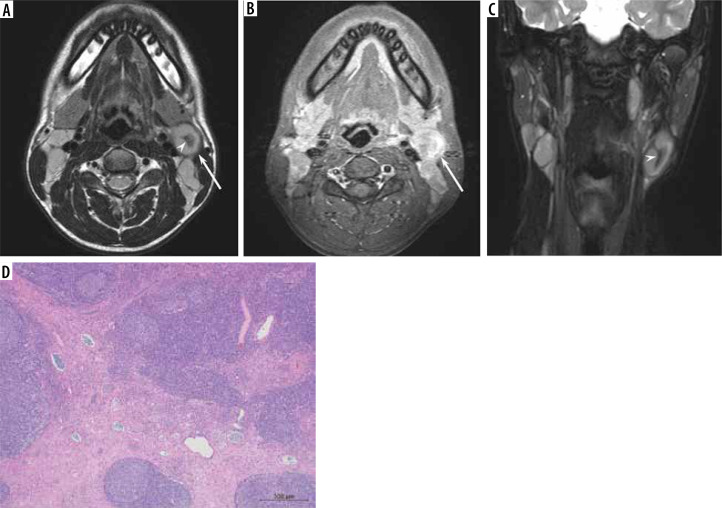
Results: The maximum diameter (22.4 ± 6.9 vs. 33.3 ± 16.0 mm, p < 0.01), minimum diameter (15.8 ± 3.6 vs. 22.3 ± 8.5 mm, p < 0.01), and SUVmax (6.9 ± 2.7 vs. 12.8 ± 8.0, p < 0.01) of the lesion were lower in reactive lymphadenitis than in nodal lymphoma, respectively. T2-hypointense-thickened capsules > 2 mm (46% vs. 14%, p < 0.05) and T2-hypointense areas converging to the periphery (15% vs. 0%, p < 0.05) were more frequently observed in reactive lymphadenitis than in nodal lymphoma, respectively. Hilum of nodes on T2-weighted images (54% vs. 22%, p < 0.05) and diffusion-weighted images (69% vs. 30%, p < 0.05) were more frequently demonstrated in reactive lymphadenitis than in nodal lymphoma, respectively.
Conclusions: Reactive lymphadenitis had a smaller size and lower SUVmax. The presence of T2-hypointense-thickened capsules, T2-hypointense areas converging to the periphery, and hilum of nodes were signs of reactive lymphadenitis.
目的:本研究旨在比较磁共振成像(MRI)和18f -氟脱氧葡萄糖(FDG)-正电子发射断层扫描/计算机断层扫描(PET/CT)对头颈部反应性淋巴结炎与淋巴结性淋巴瘤的鉴别表现。材料和方法:本研究纳入138例经组织病理学证实的颈部淋巴结病患者,其中反应性淋巴结炎35例,结性淋巴瘤103例,活检前行颈部MRI (n = 63)和/或18F-FDG-PET/CT (n = 123)检查。回顾性分析和比较两种病理的定量和定性MRI结果及最大标准化摄取值(SUVmax)。结果:反应性淋巴结炎的最大直径(22.4±6.9比33.3±16.0 mm, p < 0.01)、最小直径(15.8±3.6比22.3±8.5 mm, p < 0.01)、SUVmax(6.9±2.7比12.8±8.0,p < 0.01)均低于淋巴结性淋巴瘤。反应性淋巴结炎患者比淋巴结性淋巴瘤患者更常出现t2 -低信号区增厚的胶囊bbb2.0 mm (46% vs. 14%, p < 0.05)和t2 -低信号区向周围聚集(15% vs. 0%, p < 0.05)。t2加权图像上淋巴结门部(54%对22%,p < 0.05)和弥漫性加权图像(69%对30%,p < 0.05)在反应性淋巴结炎中比在淋巴结淋巴瘤中更常见。结论:反应性淋巴结炎体积较小,SUVmax较低。t2 -低信号区增厚囊、t2 -低信号区向外周会聚、淋巴结门部为反应性淋巴结炎的征象。


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
