Ceylan Avcı, Meltem Kaşıkçı, Banu Lebe, Sevgi Akarsu, Turna İlknur
{"title":"Diagnostic Performance of Dermoscopy for Distinguishing Early Melanomas and Intermediate Melanocytic Lesions From Low-Grade Dysplastic Nevi.","authors":"Ceylan Avcı, Meltem Kaşıkçı, Banu Lebe, Sevgi Akarsu, Turna İlknur","doi":"10.1177/12034754251325508","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Early melanomas, dysplastic melanocytic nevi, and melanocytic tumours of uncertain malignant potential (MELTUMPs) reveal similar clinic and dermoscopic findings leading to underdiagnosis of malign lesions or unnecessary excision of benign ones. High-grade dysplastic nevi and MELTUMPs in the intermediate category should be recognized and completely excised.</p><p><strong>Objectives: </strong>We evaluated the diagnostic performance of pattern analysis, ABCD rule, colour, architecture, symmetry, and homogeneity algorithm, melanoma-specific structures and asymmetry of dermoscopic features in distinguishing early melanomas, high-grade dysplastic nevi, and MELTUMPs from low-grade dysplastic nevi.</p><p><strong>Methods: </strong>We retrospectively assessed dermoscopic images blindly to the histopathological diagnoses in a university hospital.</p><p><strong>Results: </strong>One hundred forty histopathologically confirmed melanocytic lesions were included (93 low-grade dysplastic nevi, 26 thin melanomas, 17 high-grade dysplastic nevi, and 4 MELTUMPs). All dermoscopic methods had poor diagnostic performance in early melanomas and intermediate melanocytic lesions. In the multivariate analyses of dermoscopic findings, the atypical pigment network (OR: 3.58, 95% CI: 1.31-9.72), asymmetry of globules (OR: 3.17, 95% CI: 1.37-7.35), streaks (OR: 6.16, 95% CI: 1.95-19.48) and homogenous structureless areas (OR: 5.92, 95% CI: 2.36-14.92) were the significant predictive factors for melanomas and intermediate melanocytic lesions. Positive predictive values of melanoma-specific structures were shiny white structures (100%), scar-like depigmentation (85.7%), blue-white veil (72.7%), atypical blotch (72.2%), and negative pigment network (71.4%).</p><p><strong>Conclusions: </strong>Shiny white structures, atypical network, asymmetry of globules, streaks, and homogeneous structureless areas were the most significant dermoscopic findings in discriminating early melanomas and intermediate melanocytic lesions from low-grade dysplastic nevi.</p>","PeriodicalId":15403,"journal":{"name":"Journal of Cutaneous Medicine and Surgery","volume":" ","pages":"452-459"},"PeriodicalIF":3.9000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12432283/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cutaneous Medicine and Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/12034754251325508","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/12 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"DERMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Early melanomas, dysplastic melanocytic nevi, and melanocytic tumours of uncertain malignant potential (MELTUMPs) reveal similar clinic and dermoscopic findings leading to underdiagnosis of malign lesions or unnecessary excision of benign ones. High-grade dysplastic nevi and MELTUMPs in the intermediate category should be recognized and completely excised.
Objectives: We evaluated the diagnostic performance of pattern analysis, ABCD rule, colour, architecture, symmetry, and homogeneity algorithm, melanoma-specific structures and asymmetry of dermoscopic features in distinguishing early melanomas, high-grade dysplastic nevi, and MELTUMPs from low-grade dysplastic nevi.
Methods: We retrospectively assessed dermoscopic images blindly to the histopathological diagnoses in a university hospital.
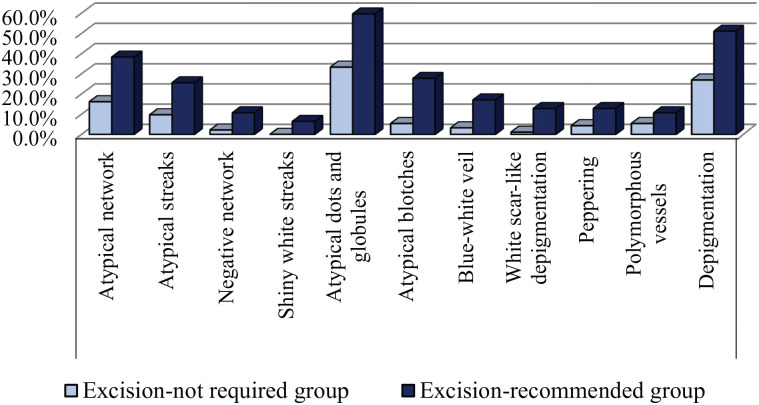
Results: One hundred forty histopathologically confirmed melanocytic lesions were included (93 low-grade dysplastic nevi, 26 thin melanomas, 17 high-grade dysplastic nevi, and 4 MELTUMPs). All dermoscopic methods had poor diagnostic performance in early melanomas and intermediate melanocytic lesions. In the multivariate analyses of dermoscopic findings, the atypical pigment network (OR: 3.58, 95% CI: 1.31-9.72), asymmetry of globules (OR: 3.17, 95% CI: 1.37-7.35), streaks (OR: 6.16, 95% CI: 1.95-19.48) and homogenous structureless areas (OR: 5.92, 95% CI: 2.36-14.92) were the significant predictive factors for melanomas and intermediate melanocytic lesions. Positive predictive values of melanoma-specific structures were shiny white structures (100%), scar-like depigmentation (85.7%), blue-white veil (72.7%), atypical blotch (72.2%), and negative pigment network (71.4%).
Conclusions: Shiny white structures, atypical network, asymmetry of globules, streaks, and homogeneous structureless areas were the most significant dermoscopic findings in discriminating early melanomas and intermediate melanocytic lesions from low-grade dysplastic nevi.
期刊介绍:
Journal of Cutaneous Medicine and Surgery (JCMS) aims to reflect the state of the art in cutaneous biology and dermatology by providing original scientific writings, as well as a complete critical review of the dermatology literature for clinicians, trainees, and academicians. JCMS endeavours to bring readers cutting edge dermatologic information in two distinct formats. Part of each issue features scholarly research and articles on issues of basic and applied science, insightful case reports, comprehensive continuing medical education, and in depth reviews, all of which provide theoretical framework for practitioners to make sound practical decisions. The evolving field of dermatology is highlighted through these articles. In addition, part of each issue is dedicated to making the most important developments in dermatology easily accessible to the clinician by presenting well-chosen, well-written, and highly organized information in a format that is interesting, clearly presented, and useful to patient care.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
