Danilo Coco, Silvana Leanza, Massimo Giuseppe Viola, Desideria Coco
{"title":"Systematic Review of Robotic Nephrectomy for Kidney Cancer.","authors":"Danilo Coco, Silvana Leanza, Massimo Giuseppe Viola, Desideria Coco","doi":"10.15586/jkc.v12i1.372","DOIUrl":null,"url":null,"abstract":"<p><p>Robotic nephrectomy has become an increasingly preferred surgical technique for managing renal cell carcinoma (RCC). This review aims to systematically evaluate existing literature on the safety, efficacy, clinical outcomes, and associated costs of robotic nephrectomy, especially in relation to tumor dimensions and other pertinent patient factors. Following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, we performed an extensive literature search across major databases (PubMed, Scopus, and Cochrane Library) from inception to October 2023. The inclusion criteria encompassed randomized controlled trials (RCTs), cohort studies, and case-control studies that compared robotic nephrectomy with open or laparoscopic nephrectomy. Outcomes analyzed included operative time, intraoperative blood loss, complication rates, length of hospital stay, oncological outcomes, and cost-effectiveness. The Egger test was used to assess publication bias. The review incorporated 30 studies involving 5,432 patients who underwent robotic nephrectomy. Key findings indicated that robotic nephrectomy resulted in significantly reduced intraoperative blood loss (mean difference of -85 mL; p < 0.001) and shorter hospital stays (mean difference of -1.3 days). Tumor size had a notable impact on surgical outcomes, with larger tumors (≥7 cm) being associated with prolonged operative times and slightly higher complication rates. Robotic nephrectomy was also associated with higher costs compared to conventional surgical techniques; however, reduced readmission rates offset some of these costs. Oncological outcomes for robotic nephrectomy were comparable to those of open nephrectomy. Robotic nephrectomy is a safe and effective approach for kidney cancer that demonstrates advantages in perioperative recovery and surgical precision, particularly for smaller tumors. While costs may be higher, the clinical benefits and potential long-term savings from decreased postoperative complications recommend its use. Further high-quality RCTs are essential to validate these findings.</p>","PeriodicalId":44291,"journal":{"name":"Journal of Kidney Cancer and VHL","volume":"12 1","pages":"29-35"},"PeriodicalIF":1.9000,"publicationDate":"2025-03-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11909633/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Kidney Cancer and VHL","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.15586/jkc.v12i1.372","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
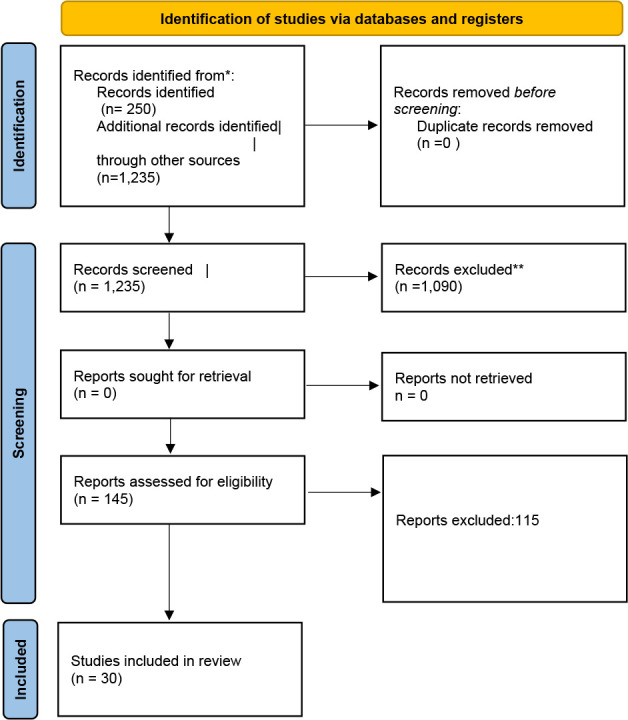
Robotic nephrectomy has become an increasingly preferred surgical technique for managing renal cell carcinoma (RCC). This review aims to systematically evaluate existing literature on the safety, efficacy, clinical outcomes, and associated costs of robotic nephrectomy, especially in relation to tumor dimensions and other pertinent patient factors. Following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, we performed an extensive literature search across major databases (PubMed, Scopus, and Cochrane Library) from inception to October 2023. The inclusion criteria encompassed randomized controlled trials (RCTs), cohort studies, and case-control studies that compared robotic nephrectomy with open or laparoscopic nephrectomy. Outcomes analyzed included operative time, intraoperative blood loss, complication rates, length of hospital stay, oncological outcomes, and cost-effectiveness. The Egger test was used to assess publication bias. The review incorporated 30 studies involving 5,432 patients who underwent robotic nephrectomy. Key findings indicated that robotic nephrectomy resulted in significantly reduced intraoperative blood loss (mean difference of -85 mL; p < 0.001) and shorter hospital stays (mean difference of -1.3 days). Tumor size had a notable impact on surgical outcomes, with larger tumors (≥7 cm) being associated with prolonged operative times and slightly higher complication rates. Robotic nephrectomy was also associated with higher costs compared to conventional surgical techniques; however, reduced readmission rates offset some of these costs. Oncological outcomes for robotic nephrectomy were comparable to those of open nephrectomy. Robotic nephrectomy is a safe and effective approach for kidney cancer that demonstrates advantages in perioperative recovery and surgical precision, particularly for smaller tumors. While costs may be higher, the clinical benefits and potential long-term savings from decreased postoperative complications recommend its use. Further high-quality RCTs are essential to validate these findings.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
