Laura J Bonnett, Thomas Spain, Alexandra Hunt, Jane L Hutton, Victoria Watson, Anthony G Marson, John Blakey
{"title":"Guide to evaluating performance of prediction models for recurrent clinical events.","authors":"Laura J Bonnett, Thomas Spain, Alexandra Hunt, Jane L Hutton, Victoria Watson, Anthony G Marson, John Blakey","doi":"10.1186/s41512-025-00187-7","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Many chronic conditions, such as epilepsy and asthma, are typified by recurrent events-repeated acute deterioration events of a similar type. Statistical models for these conditions often focus on evaluating the time to the first event. They therefore do not make use of data available on all events. Statistical models for recurrent events exist, but it is not clear how best to evaluate their performance. We compare the relative performance of statistical models for analysing recurrent events for epilepsy and asthma.</p><p><strong>Methods: </strong>We studied two clinical exemplars of common and infrequent events: asthma exacerbations using the Optimum Patient Clinical Research Database, and epileptic seizures using data from the Standard versus New Antiepileptic Drug Study. In both cases, count-based models (negative binomial and zero-inflated negative binomial) and variants on the Cox model (Andersen-Gill and Prentice, Williams and Peterson) were used to assess the risk of recurrence (of exacerbations or seizures respectively). Performance of models was evaluated via numerical (root mean square prediction error, mean absolute prediction error, and prediction bias) and graphical (calibration plots and Bland-Altman plots) approaches.</p><p><strong>Results: </strong>The performance of the prediction models for asthma and epilepsy recurrent events could be evaluated via the selected numerical and graphical measures. For both the asthma and epilepsy exemplars, the Prentice, Williams and Peterson model showed the closest agreement between predicted and observed outcomes.</p><p><strong>Conclusion: </strong>Inappropriate models can lead to incorrect conclusions which disadvantage patients. Therefore, prediction models for outcomes associated with chronic conditions should include all repeated events. Such models can be evaluated via the promoted numerical and graphical approaches alongside modified calibration measures.</p>","PeriodicalId":72800,"journal":{"name":"Diagnostic and prognostic research","volume":"9 1","pages":"6"},"PeriodicalIF":3.9000,"publicationDate":"2025-03-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11912649/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Diagnostic and prognostic research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s41512-025-00187-7","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Many chronic conditions, such as epilepsy and asthma, are typified by recurrent events-repeated acute deterioration events of a similar type. Statistical models for these conditions often focus on evaluating the time to the first event. They therefore do not make use of data available on all events. Statistical models for recurrent events exist, but it is not clear how best to evaluate their performance. We compare the relative performance of statistical models for analysing recurrent events for epilepsy and asthma.
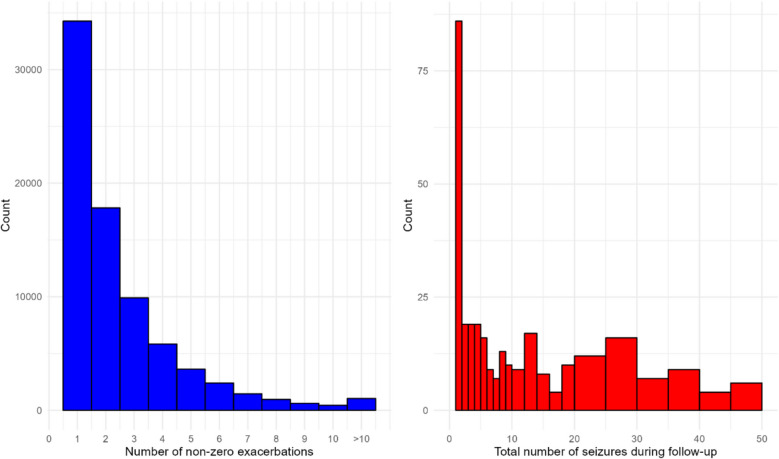
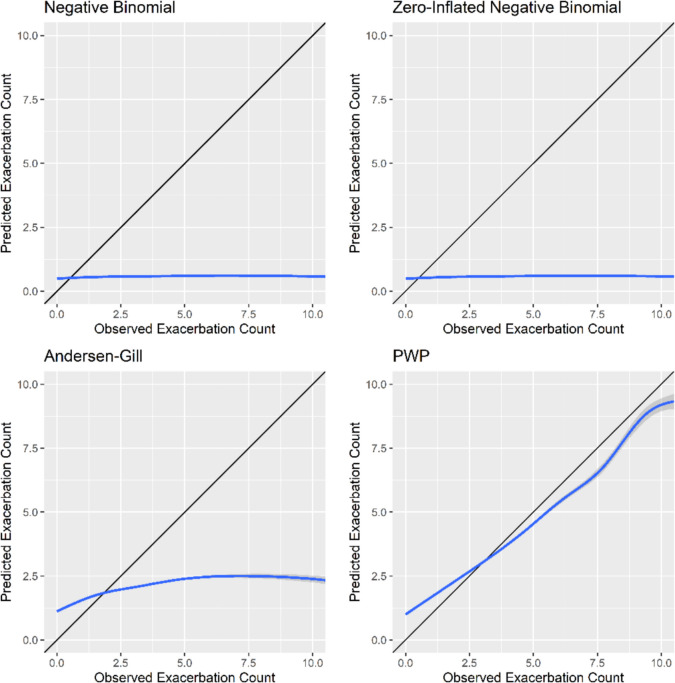
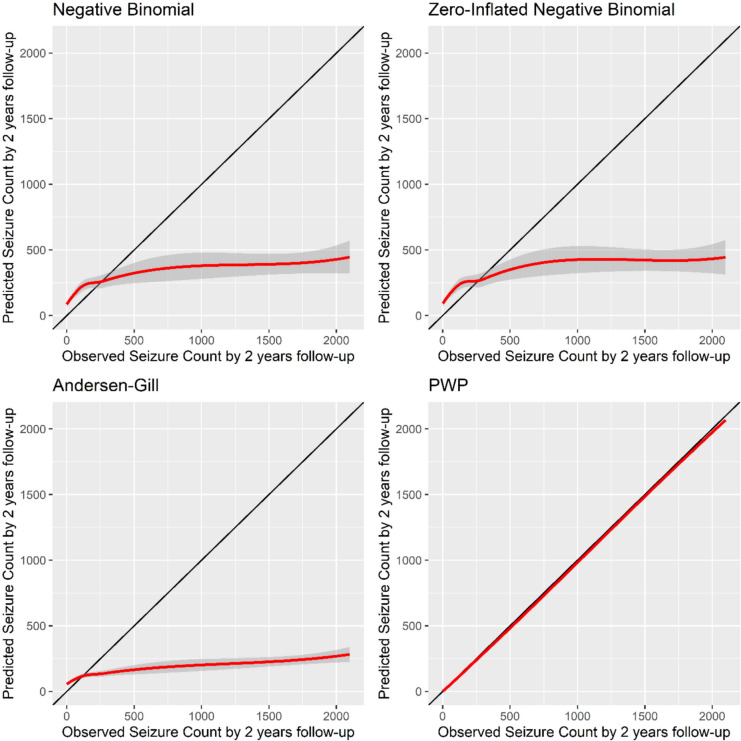
Methods: We studied two clinical exemplars of common and infrequent events: asthma exacerbations using the Optimum Patient Clinical Research Database, and epileptic seizures using data from the Standard versus New Antiepileptic Drug Study. In both cases, count-based models (negative binomial and zero-inflated negative binomial) and variants on the Cox model (Andersen-Gill and Prentice, Williams and Peterson) were used to assess the risk of recurrence (of exacerbations or seizures respectively). Performance of models was evaluated via numerical (root mean square prediction error, mean absolute prediction error, and prediction bias) and graphical (calibration plots and Bland-Altman plots) approaches.
Results: The performance of the prediction models for asthma and epilepsy recurrent events could be evaluated via the selected numerical and graphical measures. For both the asthma and epilepsy exemplars, the Prentice, Williams and Peterson model showed the closest agreement between predicted and observed outcomes.
Conclusion: Inappropriate models can lead to incorrect conclusions which disadvantage patients. Therefore, prediction models for outcomes associated with chronic conditions should include all repeated events. Such models can be evaluated via the promoted numerical and graphical approaches alongside modified calibration measures.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
