{"title":"Impact of an innovative case-based payment reform on hospital cost variation: insights from cerebral infarction inpatients in China.","authors":"Yining Wang, Shiting Liu, Xinyu Zhang, Haifeng Ma, Xiaohua Ying","doi":"10.1186/s12939-025-02447-w","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Variations in hospital costs often indicate deficiency in efficient and standardised care. Case-based provider payment systems are utilised globally to address these issues. In China, an innovative case-based payment scheme called the Diagnosis-Intervention Packet (DIP) under the global budget framework has been progressively implemented. However, evidence regarding its effectiveness and potential mechanisms underlying its impact is limited. This study aimed to investigate the impact of DIP reform on hospital cost variations among patients with cerebral infarction (CI) and to explore potential pathways through quality-cost trade-offs.</p><p><strong>Methods: </strong>This cross-sectional study analysed de-identified discharge records of patients from City G, China, between January 2018 and December 2022. The study included 293,255 cases discharged with CI from 185 hospitals. Interrupted time series models were used to assess the overall and heterogeneous impacts on hospital cost variations, measured by the coefficient of variation (CV) and interquartile range (IQR) of the hospital-level average cost per case. The contribution of each itemised cost was quantified using grey relational analysis. Quality measures were compared across hospital groups organised based on the hospitals' relative cost rankings.</p><p><strong>Results: </strong>Following the DIP reform, a significant immediate decline of 0.137 (p = 0.031) was observed in the CV. The quarterly trends in CV decreased by 0.001 (p = 0.954) and IQR by 103.40 RMB ($14.48; p = 0.389). Subgroup analyses found significant reductions in secondary hospitals, surgical groups, and medication costs, with medication costs aligning the most with the total change. Given hospital convergence toward the average cost level, no association between costs and quality was observed. Hospitals transitioning from the high-cost category experienced a reduction in in-hospital mortality (-0.5%). Similarly, those moving from the average- to low-cost category demonstrated decreased mortality (-0.7%) and complications (-0.5%).</p><p><strong>Conclusions: </strong>Our findings revealed a concentrated distribution of post-reform hospital costs without compromising quality. These findings suggest the effectiveness of case-based payment systems in reducing hospital cost variations and improving healthcare efficiency, potentially because providers adopt more standardised behaviours in response to incentive changes. This study offers insights to other countries on payment systems as leverage to achieve efficient, equitable, and high-value care.</p>","PeriodicalId":13745,"journal":{"name":"International Journal for Equity in Health","volume":"24 1","pages":"78"},"PeriodicalIF":4.1000,"publicationDate":"2025-03-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11921486/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal for Equity in Health","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12939-025-02447-w","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Variations in hospital costs often indicate deficiency in efficient and standardised care. Case-based provider payment systems are utilised globally to address these issues. In China, an innovative case-based payment scheme called the Diagnosis-Intervention Packet (DIP) under the global budget framework has been progressively implemented. However, evidence regarding its effectiveness and potential mechanisms underlying its impact is limited. This study aimed to investigate the impact of DIP reform on hospital cost variations among patients with cerebral infarction (CI) and to explore potential pathways through quality-cost trade-offs.
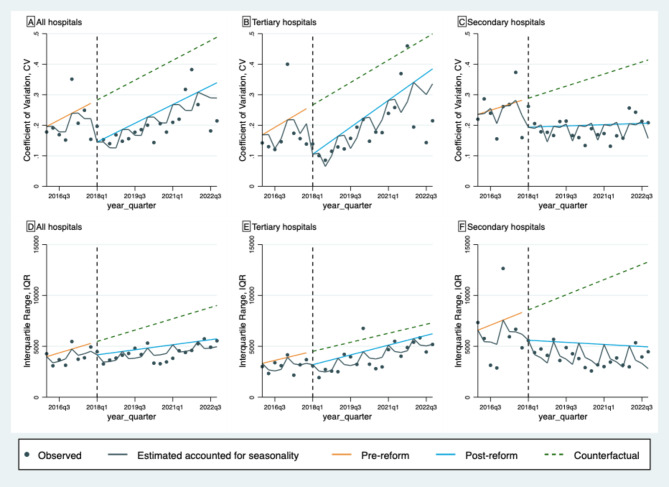
Methods: This cross-sectional study analysed de-identified discharge records of patients from City G, China, between January 2018 and December 2022. The study included 293,255 cases discharged with CI from 185 hospitals. Interrupted time series models were used to assess the overall and heterogeneous impacts on hospital cost variations, measured by the coefficient of variation (CV) and interquartile range (IQR) of the hospital-level average cost per case. The contribution of each itemised cost was quantified using grey relational analysis. Quality measures were compared across hospital groups organised based on the hospitals' relative cost rankings.
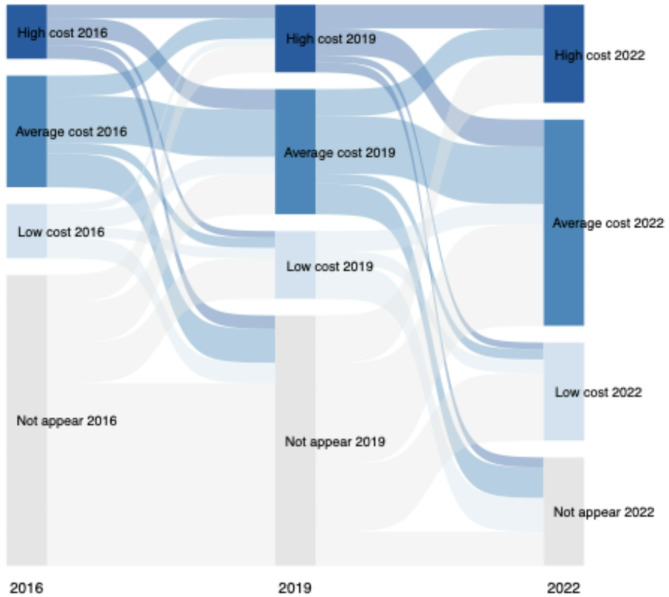
Results: Following the DIP reform, a significant immediate decline of 0.137 (p = 0.031) was observed in the CV. The quarterly trends in CV decreased by 0.001 (p = 0.954) and IQR by 103.40 RMB ($14.48; p = 0.389). Subgroup analyses found significant reductions in secondary hospitals, surgical groups, and medication costs, with medication costs aligning the most with the total change. Given hospital convergence toward the average cost level, no association between costs and quality was observed. Hospitals transitioning from the high-cost category experienced a reduction in in-hospital mortality (-0.5%). Similarly, those moving from the average- to low-cost category demonstrated decreased mortality (-0.7%) and complications (-0.5%).
Conclusions: Our findings revealed a concentrated distribution of post-reform hospital costs without compromising quality. These findings suggest the effectiveness of case-based payment systems in reducing hospital cost variations and improving healthcare efficiency, potentially because providers adopt more standardised behaviours in response to incentive changes. This study offers insights to other countries on payment systems as leverage to achieve efficient, equitable, and high-value care.
期刊介绍:
International Journal for Equity in Health is an Open Access, peer-reviewed, online journal presenting evidence relevant to the search for, and attainment of, equity in health across and within countries. International Journal for Equity in Health aims to improve the understanding of issues that influence the health of populations. This includes the discussion of political, policy-related, economic, social and health services-related influences, particularly with regard to systematic differences in distributions of one or more aspects of health in population groups defined demographically, geographically, or socially.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
