Peter Paul F Klein, Sigur Gouwens, Katalin Katona, Niek Stadhouders, Talitha L Feenstra
{"title":"Using microdata as a basis for long term projections of hospital care spending: the added value of more detailed information.","authors":"Peter Paul F Klein, Sigur Gouwens, Katalin Katona, Niek Stadhouders, Talitha L Feenstra","doi":"10.1186/s13561-025-00607-w","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Component-based projections are commonly used to predict future growth in healthcare spending. The current study aimed to compare pure component-based projections to projections using microlevel data to investigate their added value.</p><p><strong>Methods: </strong>The microdata was used to find disease-specific time trends in the number of patients that use hospital care and in annual per patient hospital spending (APHS). Total expenditure projections were then based on APHS and hospital use per disease category combined with demographic projections. As comparator, we used projections with a composite growth term derived from total spending time trends. Furthermore, extensive uncertainty analyses were performed.</p><p><strong>Results: </strong>Time -trends were present both in hospital care usage and in annual per patient hospital spending (APHS) for most disease groups. What is known as the \"residual growth\" category in many projections of healthcare spending can be split into these two time- trends, offering more insight into their sources. The advantage of explicit modeling as done in this paper is that trends in usage and per patient spending can be separated. The use of microdata allowed further refinement of component-based models for projections in healthcare spending and a more elaborate analysis of uncertainty surrounding these projections.</p><p><strong>Conclusions: </strong>We found time trends in both hospital care usage and APHS in most disease groups. Incorporating these trends into cost projections for various disease groups results in more conservative estimates of future hospital spending compared to merely using demographic projections of per capita costs and adjusting them for observed historical growth. The use of microdata for component-based modelling has benefits but also downsides. A positive side of using microlevel data is that individuals could be followed over multiple years, a downside was the vast amount of computing power and time needed to perform these extensive analyses. Our results could support policy makers to adjust for hospital (staffing) capacity not purely on demographic changes but also based on observed trends in the use of specific types of hospital care, per disease.</p>","PeriodicalId":46936,"journal":{"name":"Health Economics Review","volume":"15 1","pages":"25"},"PeriodicalIF":3.3000,"publicationDate":"2025-03-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11921507/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Health Economics Review","FirstCategoryId":"96","ListUrlMain":"https://doi.org/10.1186/s13561-025-00607-w","RegionNum":3,"RegionCategory":"经济学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ECONOMICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Component-based projections are commonly used to predict future growth in healthcare spending. The current study aimed to compare pure component-based projections to projections using microlevel data to investigate their added value.
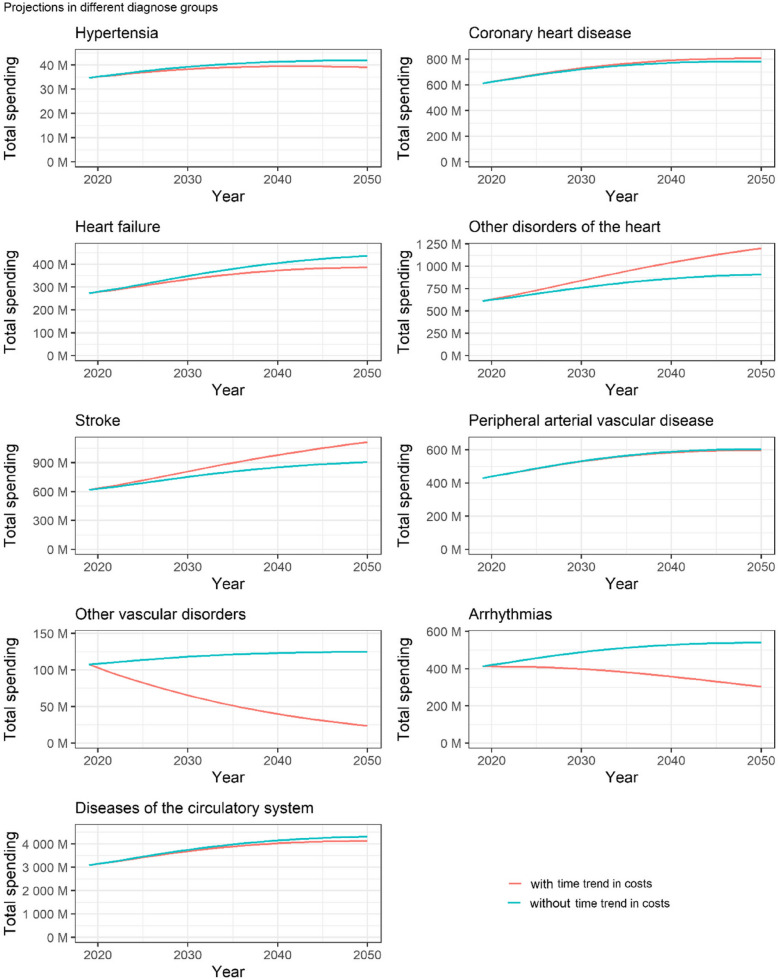
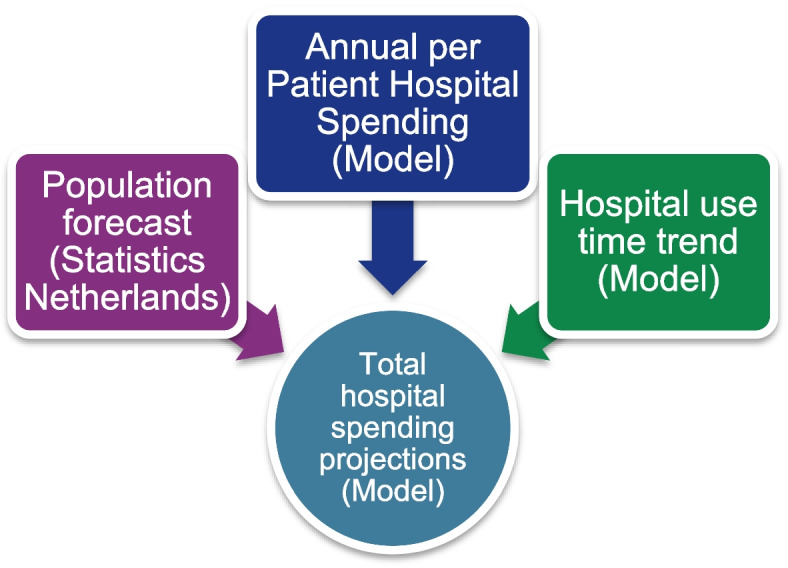
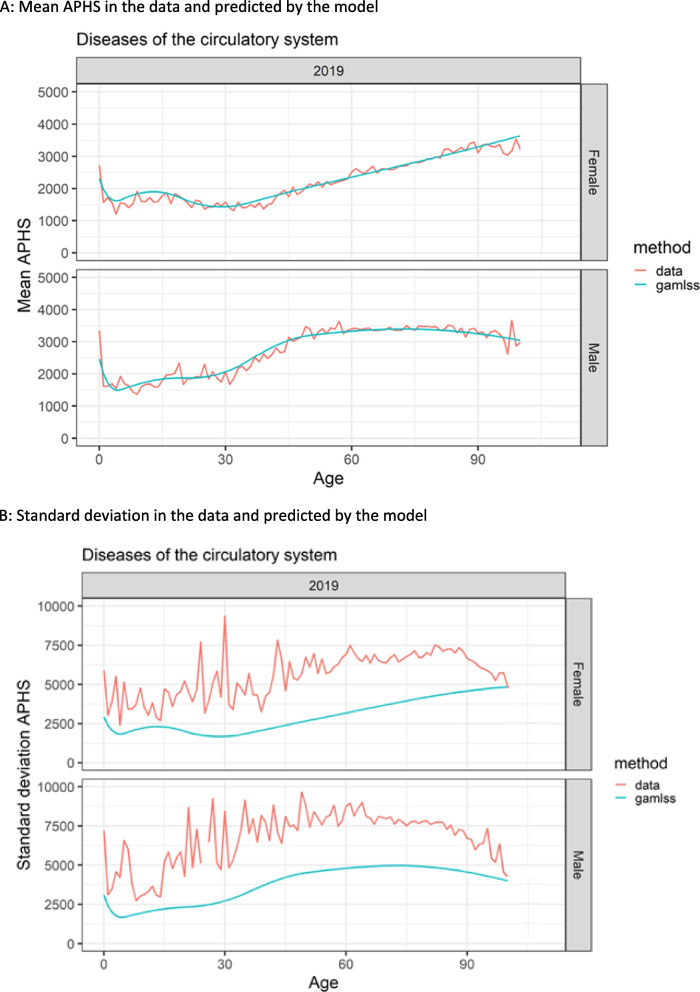
Methods: The microdata was used to find disease-specific time trends in the number of patients that use hospital care and in annual per patient hospital spending (APHS). Total expenditure projections were then based on APHS and hospital use per disease category combined with demographic projections. As comparator, we used projections with a composite growth term derived from total spending time trends. Furthermore, extensive uncertainty analyses were performed.
Results: Time -trends were present both in hospital care usage and in annual per patient hospital spending (APHS) for most disease groups. What is known as the "residual growth" category in many projections of healthcare spending can be split into these two time- trends, offering more insight into their sources. The advantage of explicit modeling as done in this paper is that trends in usage and per patient spending can be separated. The use of microdata allowed further refinement of component-based models for projections in healthcare spending and a more elaborate analysis of uncertainty surrounding these projections.
Conclusions: We found time trends in both hospital care usage and APHS in most disease groups. Incorporating these trends into cost projections for various disease groups results in more conservative estimates of future hospital spending compared to merely using demographic projections of per capita costs and adjusting them for observed historical growth. The use of microdata for component-based modelling has benefits but also downsides. A positive side of using microlevel data is that individuals could be followed over multiple years, a downside was the vast amount of computing power and time needed to perform these extensive analyses. Our results could support policy makers to adjust for hospital (staffing) capacity not purely on demographic changes but also based on observed trends in the use of specific types of hospital care, per disease.
期刊介绍:
Health Economics Review is an international high-quality journal covering all fields of Health Economics. A broad range of theoretical contributions, empirical studies and analyses of health policy with a health economic focus will be considered for publication. Its scope includes macro- and microeconomics of health care financing, health insurance and reimbursement as well as health economic evaluation, health services research and health policy analysis. Further research topics are the individual and institutional aspects of health care management and the growing importance of health care in developing countries.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
