Aman Pal, Emmanuel Aydin-Ghormoz, Swati Mehta, M J Hajianpour, Emily Gaine, Muhammad Ali Zia, Elie Tannous, Andrea Lightle, Krishnakumar Hongalgi
{"title":"Atypical presentation of H1N1-induced thrombotic microangiopathy with CD46 gene mutation\u2029.","authors":"Aman Pal, Emmanuel Aydin-Ghormoz, Swati Mehta, M J Hajianpour, Emily Gaine, Muhammad Ali Zia, Elie Tannous, Andrea Lightle, Krishnakumar Hongalgi","doi":"10.5414/CNCS111525","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Thrombotic microangiopathy (TMA) is a pathological description which clinically presents with thrombocytopenia, microangiopathic hemolytic anemia (MAHA), and organ dysfunction. The etiology of TMA is broadly classified into four categories: primary hereditary, primary acquired, secondary, and infection associated. H1N1 influenza is a rare etiology of complement-mediated TMA (CM-TMA) with there being under 30 cases reported to date, and its odd presentation with hemoptysis making it a challenge to diagnose.</p><p><strong>Case presentation: </strong>We present a case of a Caucasian female in her 20s presenting to the hospital with a viral prodrome in setting of a new acute kidney injury (creatinine 8.2 mg/dL), thrombocytopenia (platelet count 14,000/mm<sup>3</sup>), and H1N1 influenza positive. She developed hemoptysis the next day, with no respiratory distress. Rheumatology work-up for antineutrophilic cytoplasmic antibodies (ANCA), anti-glomerular basement membrane (anti-GBM), and antiphospholipid syndrome (APS) antibodies was negative. CT chest was also negative for pulmonary hemorrhage. Plasma exchange was started empirically until ADAMTS13 activity returned normal (120%), and she was further commenced on eculizumab after an atypical hemolytic uremic syndrome (aHUS)/TMA/Complement 3 Glomerulopathy (C3G) gene panel was sent. Molecular studies revealed a splice site variant of MCP/CD46 gene, which was reiterated on a renal biopsy. The patient was counselled on the genetic results, including predisposition to future events and the importance of long-term eculizumab treatment.</p><p><strong>Discussion: </strong>CM-TMA is a consequence of alternative pathway dysregulation, commonly associated with genetic mutations which could phenotypically be unmasked by infections, such as influenza virus.</p><p><strong>Conclusion: </strong>Our case highlights the importance of keeping a broad differential beyond classic pulmonary-renal syndromes in patients presenting with hemoptysis and TMA, while understanding the pathophysiology of infections unmasking genetic mutations in CM-TMA.\u2029.</p>","PeriodicalId":510898,"journal":{"name":"Clinical nephrology. Case studies","volume":"13 ","pages":"28-36"},"PeriodicalIF":0.0000,"publicationDate":"2025-03-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11924108/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical nephrology. Case studies","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5414/CNCS111525","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
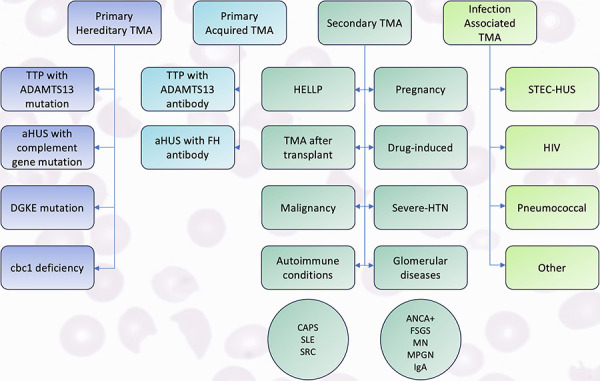
Introduction: Thrombotic microangiopathy (TMA) is a pathological description which clinically presents with thrombocytopenia, microangiopathic hemolytic anemia (MAHA), and organ dysfunction. The etiology of TMA is broadly classified into four categories: primary hereditary, primary acquired, secondary, and infection associated. H1N1 influenza is a rare etiology of complement-mediated TMA (CM-TMA) with there being under 30 cases reported to date, and its odd presentation with hemoptysis making it a challenge to diagnose.
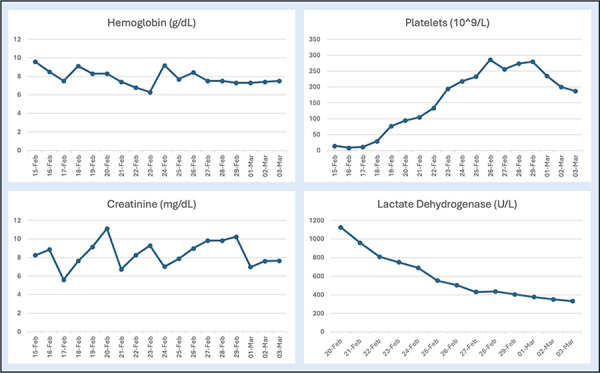
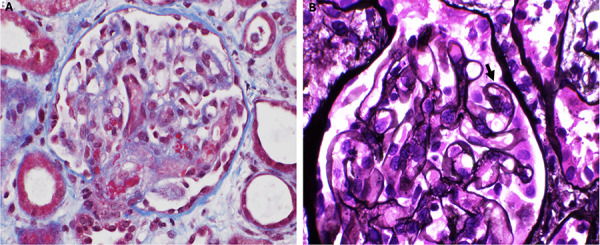
Case presentation: We present a case of a Caucasian female in her 20s presenting to the hospital with a viral prodrome in setting of a new acute kidney injury (creatinine 8.2 mg/dL), thrombocytopenia (platelet count 14,000/mm3), and H1N1 influenza positive. She developed hemoptysis the next day, with no respiratory distress. Rheumatology work-up for antineutrophilic cytoplasmic antibodies (ANCA), anti-glomerular basement membrane (anti-GBM), and antiphospholipid syndrome (APS) antibodies was negative. CT chest was also negative for pulmonary hemorrhage. Plasma exchange was started empirically until ADAMTS13 activity returned normal (120%), and she was further commenced on eculizumab after an atypical hemolytic uremic syndrome (aHUS)/TMA/Complement 3 Glomerulopathy (C3G) gene panel was sent. Molecular studies revealed a splice site variant of MCP/CD46 gene, which was reiterated on a renal biopsy. The patient was counselled on the genetic results, including predisposition to future events and the importance of long-term eculizumab treatment.
Discussion: CM-TMA is a consequence of alternative pathway dysregulation, commonly associated with genetic mutations which could phenotypically be unmasked by infections, such as influenza virus.
Conclusion: Our case highlights the importance of keeping a broad differential beyond classic pulmonary-renal syndromes in patients presenting with hemoptysis and TMA, while understanding the pathophysiology of infections unmasking genetic mutations in CM-TMA. .


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
