W Frank Peacock, Joseph Varon, Ramin Ebrahimi, Lala Dunbar, Charles V Pollack
{"title":"Clevidipine for severe hypertension in patients with renal dysfunction: a VELOCITY trial analysis.","authors":"W Frank Peacock, Joseph Varon, Ramin Ebrahimi, Lala Dunbar, Charles V Pollack","doi":"10.3109/08037051.2010.539317","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Acute and severe hypertension is common, especially in patients with renal dysfunction (RD). Clevidipine is a rapidly acting (t½∼1 min) intravenous (IV) dihydropyridine calcium-channel blocker metabolized by blood and tissue esterases and may be useful in patients with RD. The purpose of this analysis was to assess the safety and efficacy of clevidipine in patients with RD.</p><p><strong>Methods: </strong>VELOCITY, a multicenter open-label study of severe hypertension, enrolled 126 patients with persistent systolic blood pressure (SBP) >180 mmHg. Investigators pre-specified a SBP initial target range (ITR) for each patient to be achieved within 30 min. Blood pressure monitoring was by cuff. Clevidipine was infused via peripheral IV at 2 mg/h for at least 3 min, then doubled every 3 min as needed to a maximum of 32 mg/h (non-weight-based treat-to-target protocol). Per protocol, clevidipine was continued for at least 18 h (96 h maximum). RD was diagnosed and reported as an end-organ injury by the investigator and was defined as requiring dialysis or an initial creatinine >2.0 mg/dl. Primary endpoints were the percentage of patients within the ITR by 30 min and the percentage below the ITR after 3 min of clevidipine infusion.</p><p><strong>Results: </strong>Of the 24 patients with moderate to severe RD, most (13/24) were dialysis dependent. Forty-six percent were male, with mean age 51 ± 14 years; 63% were black and 96% had a hypertension history. Median time to achieve the ITR was 8.5 min. Almost 90% of patients reached the ITR in 30 min without evidence of overshoot and were maintained on clevidipine through 18 h. Most patients (88%) transitioned to oral antihypertensive therapy within 6 h of clevidipine termination.</p><p><strong>Conclusions: </strong>This report is the first demonstrating that clevidipine is safe and effective in RD complicated by severe hypertension. Prolonged infusion maintained blood pressure within a target range and allowed successful transition to oral therapy.</p>","PeriodicalId":8974,"journal":{"name":"Blood pressure. Supplement","volume":"1 ","pages":"20-5"},"PeriodicalIF":0.0000,"publicationDate":"2011-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.3109/08037051.2010.539317","citationCount":"15","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Blood pressure. Supplement","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3109/08037051.2010.539317","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2010/11/23 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 15
Abstract
Introduction: Acute and severe hypertension is common, especially in patients with renal dysfunction (RD). Clevidipine is a rapidly acting (t½∼1 min) intravenous (IV) dihydropyridine calcium-channel blocker metabolized by blood and tissue esterases and may be useful in patients with RD. The purpose of this analysis was to assess the safety and efficacy of clevidipine in patients with RD.
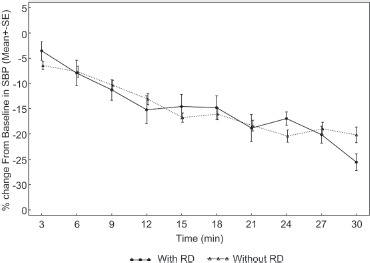
Methods: VELOCITY, a multicenter open-label study of severe hypertension, enrolled 126 patients with persistent systolic blood pressure (SBP) >180 mmHg. Investigators pre-specified a SBP initial target range (ITR) for each patient to be achieved within 30 min. Blood pressure monitoring was by cuff. Clevidipine was infused via peripheral IV at 2 mg/h for at least 3 min, then doubled every 3 min as needed to a maximum of 32 mg/h (non-weight-based treat-to-target protocol). Per protocol, clevidipine was continued for at least 18 h (96 h maximum). RD was diagnosed and reported as an end-organ injury by the investigator and was defined as requiring dialysis or an initial creatinine >2.0 mg/dl. Primary endpoints were the percentage of patients within the ITR by 30 min and the percentage below the ITR after 3 min of clevidipine infusion.
Results: Of the 24 patients with moderate to severe RD, most (13/24) were dialysis dependent. Forty-six percent were male, with mean age 51 ± 14 years; 63% were black and 96% had a hypertension history. Median time to achieve the ITR was 8.5 min. Almost 90% of patients reached the ITR in 30 min without evidence of overshoot and were maintained on clevidipine through 18 h. Most patients (88%) transitioned to oral antihypertensive therapy within 6 h of clevidipine termination.
Conclusions: This report is the first demonstrating that clevidipine is safe and effective in RD complicated by severe hypertension. Prolonged infusion maintained blood pressure within a target range and allowed successful transition to oral therapy.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
