{"title":"Triple Combination Therapy Using Metformin, Thiazolidinedione, and a GLP-1 Analog or DPP-IV Inhibitor in Patients with Type 2 Diabetes Mellitus.","authors":"Sun Woo Kim","doi":"10.4093/kdj.2010.34.6.331","DOIUrl":null,"url":null,"abstract":"<p><p>Although there is no HbA1c threshold for cardiovascular risk, the American Diabetic Association-recommended goal of HbA1c < 7.0% appears to be unacceptably high. To achieve an optimal HbA1c level goal of 6.0% or less, a high dosage of sulfonylureas and insulin would be required; the trade-off would be the common adverse effects of hypoglycemia and weight gain. In contrast, hypoglycemia is uncommon with insulin sensitizers and GLP-1 analogs, allowing the physician to titrate these drugs to maximum dosage to reduce HbA1c levels below 6.0% and they have been shown to preserve β-cell function. Lastly, weight gain is common with sulfonylurea and insulin therapy, whereas GLP-1 analogs induce weight loss and offset the weight gain associated with TZDs. A treatment paradigm shift is recommended in which combination therapy is initiated with diet/exercise, metformin (which has antiatherogenic effects and improves hepatic insulin sensitivity), a TZD (which improves insulin sensitivity and preserves β-cell function with proven durability), and a GLP-1 analog (which improves β, α-cell function and promotes weight loss) or a dipeptidyl peptidase IV inhibitor in patients with type 2 diabetes mellitus.</p>","PeriodicalId":88924,"journal":{"name":"Korean diabetes journal","volume":"34 6","pages":"331-7"},"PeriodicalIF":0.0000,"publicationDate":"2010-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.4093/kdj.2010.34.6.331","citationCount":"12","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Korean diabetes journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4093/kdj.2010.34.6.331","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2010/12/31 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 12
Abstract
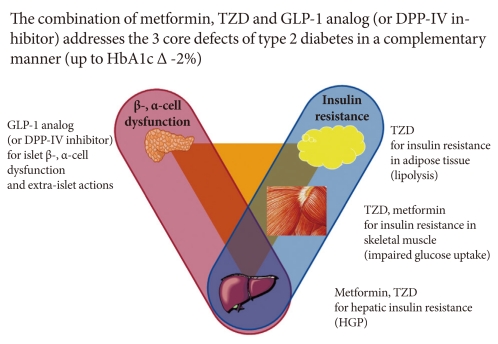
Although there is no HbA1c threshold for cardiovascular risk, the American Diabetic Association-recommended goal of HbA1c < 7.0% appears to be unacceptably high. To achieve an optimal HbA1c level goal of 6.0% or less, a high dosage of sulfonylureas and insulin would be required; the trade-off would be the common adverse effects of hypoglycemia and weight gain. In contrast, hypoglycemia is uncommon with insulin sensitizers and GLP-1 analogs, allowing the physician to titrate these drugs to maximum dosage to reduce HbA1c levels below 6.0% and they have been shown to preserve β-cell function. Lastly, weight gain is common with sulfonylurea and insulin therapy, whereas GLP-1 analogs induce weight loss and offset the weight gain associated with TZDs. A treatment paradigm shift is recommended in which combination therapy is initiated with diet/exercise, metformin (which has antiatherogenic effects and improves hepatic insulin sensitivity), a TZD (which improves insulin sensitivity and preserves β-cell function with proven durability), and a GLP-1 analog (which improves β, α-cell function and promotes weight loss) or a dipeptidyl peptidase IV inhibitor in patients with type 2 diabetes mellitus.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
