Humberto Morais, Miguel Sousa-Uva, Telmo Martins, Valdano Manuel, João Carlos Costa
{"title":"Rupture of Right Sinus of Valsalva Aneurysm into Right Cardiac Chambers: The Role of Different Imaging Modalities.","authors":"Humberto Morais, Miguel Sousa-Uva, Telmo Martins, Valdano Manuel, João Carlos Costa","doi":"10.4250/jcu.2016.24.1.84","DOIUrl":null,"url":null,"abstract":"A 25-year-old woman with no cardiovascular risk factors was admitted to our hospital with dyspnea and palpitations during the last two months. Physical examination showed blood pressure of 150/50 mm Hg and a continuous murmur across the precordium in cardiac auscultation was observed. The 12 leads electrocardiogram was normal. Chest X-ray showed a slight cardiomegaly. The transthoracic echocardiography revealed dilatation of the right cavities and a rupture of right sinus of Valsalva aneurysm (SVA) into the right atrium (Fig. 1A). The Doppler study (Fig. 1B) and transesophageal echocardiography confirmed the shunt between the right SVA and the right atrium (Fig. 1C and D, Supplementary movie 1 and 2). The rupture of right sinus of Valsalva was also demonstrated by real time 3D transesophageal echocardiography (Fig. 2A, Supplementary movie 3). Unlike transthoracic and transesophageal echocardiography which shows shunt between right SVA and right atrium, computed multidetector tomography, showed a communication between the right SVA and right cardiac chambers (right atrium and right ventricle) (blue circle, Fig. 2B). These findings were confirmed during surgery (blue arrow, Fig. 2C), and the fistula was closed (Fig. 2D). The patient's postoperative course was uneventful. The patient was discharged on the sixth post-operative day. At two years follow-up, the patient remains asymptomatic. \n \n \n \nFig. 1 \n \nA: Transthoracic echocardiography, parasternal short axis view at level of great vessels, revealed rupture of right sinus of Valsalva into the right atrium (asterisk). B, C, and D: Transesophageal echocardiography and color Doppler study confirming the ... \n \n \n \n \n \nFig. 2 \n \nA: Real time 3D transesophageal echocardiography, in zoom mode, showing rupture of right sinus of Valsalva into the right atrium (blue arrow). B: Computed multidetector tomography showing communication between the right sinus of Valsalva and right cardiac ... \n \n \n \nSVA are rare but well known congenital anomalies. They occur three times more often in males with highest incidence in Asian populations. They commonly rupture into the right ventricle or right atrium,1) rarely into the both right cardiac chambers as was observed in case presented herein. Moreover, in Africa the main complication of the SVA is the dissection into ventricular septum.2) \n \nSince the first echocardiographic description of SVA by Rothbaum et al.3) in 1974, the echocardiography plays a pivotal role in the definitive diagnosis aneurysm of the sinus of Valsalva. However, in recent years several papers have been published emphasizing the use of other imaging modalities for diagnosis of this heart condition.4),5) According to several reports, the diagnosis of SVA was made at echocardiography in 90% of cases. In present case the multidetector tomography gave more precise information showing a rare type of rupture of SVA-rupture into right cardiac chambers, and the role of multidetector tomography as additional tool for the precision of the diagnosis. \n \nIn present case the detailed anatomic and functional information obtained by these non-invasive tests were enough to guide the surgical planning without recourse to invasive studies. Invasive tests must be reserved for patients in whom the percutaneous closure of the fistula is possible, or the suspicion of coronary disease is present. Finally, given the widespread use of these new noninvasive tests, cardiologists and radiologists should be able to recognize this rare disease.","PeriodicalId":88913,"journal":{"name":"Journal of cardiovascular ultrasound","volume":"24 1","pages":"84-6"},"PeriodicalIF":0.0000,"publicationDate":"2016-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.4250/jcu.2016.24.1.84","citationCount":"3","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of cardiovascular ultrasound","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4250/jcu.2016.24.1.84","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2016/3/24 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 3
Abstract
A 25-year-old woman with no cardiovascular risk factors was admitted to our hospital with dyspnea and palpitations during the last two months. Physical examination showed blood pressure of 150/50 mm Hg and a continuous murmur across the precordium in cardiac auscultation was observed. The 12 leads electrocardiogram was normal. Chest X-ray showed a slight cardiomegaly. The transthoracic echocardiography revealed dilatation of the right cavities and a rupture of right sinus of Valsalva aneurysm (SVA) into the right atrium (Fig. 1A). The Doppler study (Fig. 1B) and transesophageal echocardiography confirmed the shunt between the right SVA and the right atrium (Fig. 1C and D, Supplementary movie 1 and 2). The rupture of right sinus of Valsalva was also demonstrated by real time 3D transesophageal echocardiography (Fig. 2A, Supplementary movie 3). Unlike transthoracic and transesophageal echocardiography which shows shunt between right SVA and right atrium, computed multidetector tomography, showed a communication between the right SVA and right cardiac chambers (right atrium and right ventricle) (blue circle, Fig. 2B). These findings were confirmed during surgery (blue arrow, Fig. 2C), and the fistula was closed (Fig. 2D). The patient's postoperative course was uneventful. The patient was discharged on the sixth post-operative day. At two years follow-up, the patient remains asymptomatic.
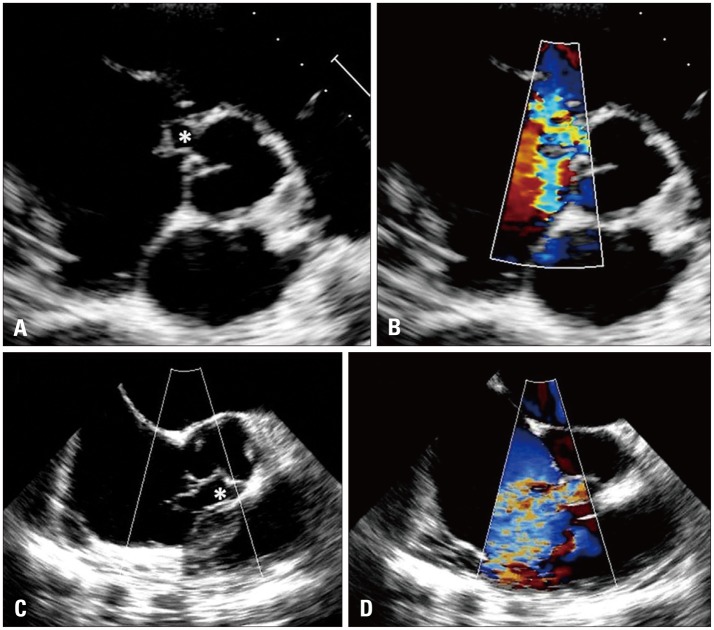
Fig. 1
A: Transthoracic echocardiography, parasternal short axis view at level of great vessels, revealed rupture of right sinus of Valsalva into the right atrium (asterisk). B, C, and D: Transesophageal echocardiography and color Doppler study confirming the ...
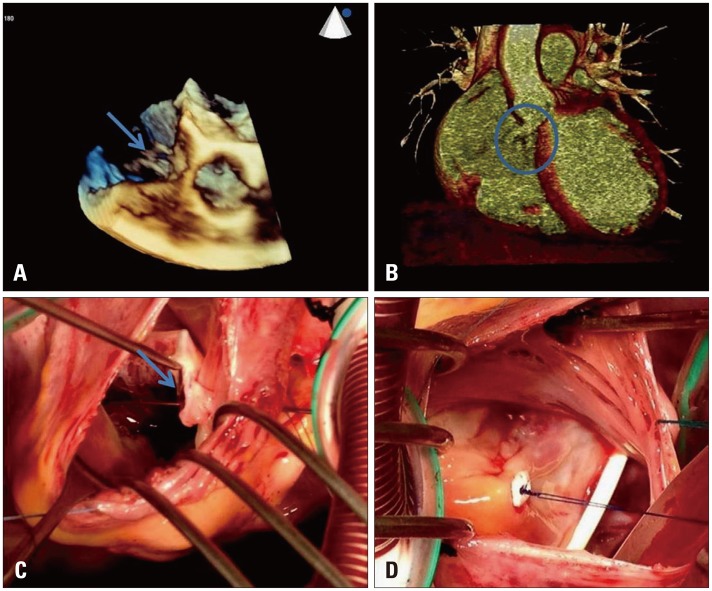
Fig. 2
A: Real time 3D transesophageal echocardiography, in zoom mode, showing rupture of right sinus of Valsalva into the right atrium (blue arrow). B: Computed multidetector tomography showing communication between the right sinus of Valsalva and right cardiac ...
SVA are rare but well known congenital anomalies. They occur three times more often in males with highest incidence in Asian populations. They commonly rupture into the right ventricle or right atrium,1) rarely into the both right cardiac chambers as was observed in case presented herein. Moreover, in Africa the main complication of the SVA is the dissection into ventricular septum.2)
Since the first echocardiographic description of SVA by Rothbaum et al.3) in 1974, the echocardiography plays a pivotal role in the definitive diagnosis aneurysm of the sinus of Valsalva. However, in recent years several papers have been published emphasizing the use of other imaging modalities for diagnosis of this heart condition.4),5) According to several reports, the diagnosis of SVA was made at echocardiography in 90% of cases. In present case the multidetector tomography gave more precise information showing a rare type of rupture of SVA-rupture into right cardiac chambers, and the role of multidetector tomography as additional tool for the precision of the diagnosis.
In present case the detailed anatomic and functional information obtained by these non-invasive tests were enough to guide the surgical planning without recourse to invasive studies. Invasive tests must be reserved for patients in whom the percutaneous closure of the fistula is possible, or the suspicion of coronary disease is present. Finally, given the widespread use of these new noninvasive tests, cardiologists and radiologists should be able to recognize this rare disease.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
