{"title":"Recurrent Acute Myocardial Infarction Caused by Intra-cardiac Metastatic Undifferentiated Pleomorphic Sarcoma during Cancer Treatment.","authors":"Sungsoo Cho, Na-Hye Myong, Tae Soo Kang","doi":"10.4250/jcu.2018.26.1.40","DOIUrl":null,"url":null,"abstract":"A 54-year-old male visited the emergency room for sudden chest pain. In his previous medical history, he had been diagnosed as left axillary undifferentiated pleomorphic sarcoma two years ago without metastasis in the heart at our hospital (Fig. 1A). Despite surgery, multiple sessions of chemotherapy and radiation therapy, the cancer had proliferated. One year after diagnosis, he had started taking pembrolizumab to target the metastasis of sarcoma. After initiation of pembrolizumab, the patient was hospitalized for sudden cardiac arrest due to acute myocardial infarction (AMI) induced by metastatic sarcoma embolus and an angioplasty had been performed at another hospital a year ago. We performed direct percutaneous coronary intervention due to ST segment elevation myocardial infarction, anterior wall and found the total occlusion of the distal left anterior descending artery (Fig. 1B). We utilized a thromboaspirate suction catheter to suction the area multiple times and obtained mucoid white tissue debris (Fig. 1C). In the final coronary angiography, the coronary flow had been completely restored (Fig. 1D). In his echocardiography six months ago, a huge mass with heterogeneous echogenicity was located in the left atrium and attached to the interatrial septum with a prolapse into the left ventricle (Fig. 2A, Supplementary Movie 1). However, the mass had significantly decreased in size on new echocardiography (Fig. 2B, Supplementary Movie 2). We compared the cytologic and immunohistochemical findings of primary axillary sarcoma with the acquired intracoronary embolus tissue. The embolus tissues were composed of discohesive round sarcoma cells and scattered pleomorphic giant cells, pISSN 1975-4612 / eISSN 2005-9655 Copyright © 2018 Korean Society of Echocardiography www.kse-jcu.org https://doi.org/10.4250/jcu.2018.26.1.40","PeriodicalId":88913,"journal":{"name":"Journal of cardiovascular ultrasound","volume":"26 1","pages":"40-42"},"PeriodicalIF":0.0000,"publicationDate":"2018-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.4250/jcu.2018.26.1.40","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of cardiovascular ultrasound","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4250/jcu.2018.26.1.40","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2018/3/28 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
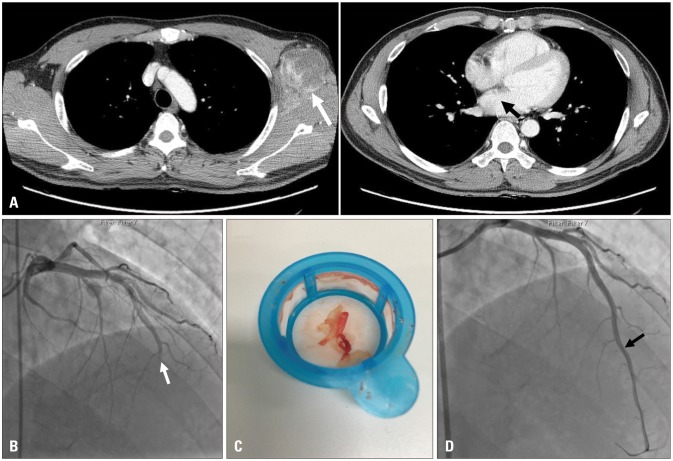
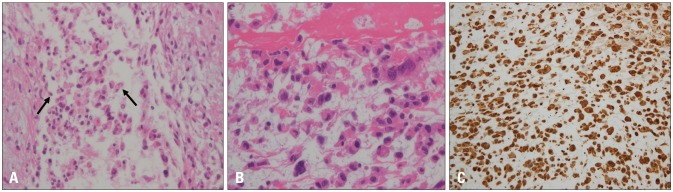
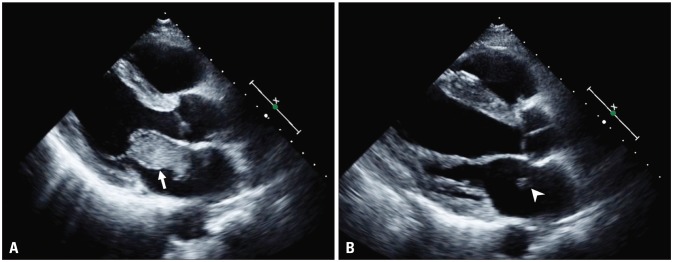
A 54-year-old male visited the emergency room for sudden chest pain. In his previous medical history, he had been diagnosed as left axillary undifferentiated pleomorphic sarcoma two years ago without metastasis in the heart at our hospital (Fig. 1A). Despite surgery, multiple sessions of chemotherapy and radiation therapy, the cancer had proliferated. One year after diagnosis, he had started taking pembrolizumab to target the metastasis of sarcoma. After initiation of pembrolizumab, the patient was hospitalized for sudden cardiac arrest due to acute myocardial infarction (AMI) induced by metastatic sarcoma embolus and an angioplasty had been performed at another hospital a year ago. We performed direct percutaneous coronary intervention due to ST segment elevation myocardial infarction, anterior wall and found the total occlusion of the distal left anterior descending artery (Fig. 1B). We utilized a thromboaspirate suction catheter to suction the area multiple times and obtained mucoid white tissue debris (Fig. 1C). In the final coronary angiography, the coronary flow had been completely restored (Fig. 1D). In his echocardiography six months ago, a huge mass with heterogeneous echogenicity was located in the left atrium and attached to the interatrial septum with a prolapse into the left ventricle (Fig. 2A, Supplementary Movie 1). However, the mass had significantly decreased in size on new echocardiography (Fig. 2B, Supplementary Movie 2). We compared the cytologic and immunohistochemical findings of primary axillary sarcoma with the acquired intracoronary embolus tissue. The embolus tissues were composed of discohesive round sarcoma cells and scattered pleomorphic giant cells, pISSN 1975-4612 / eISSN 2005-9655 Copyright © 2018 Korean Society of Echocardiography www.kse-jcu.org https://doi.org/10.4250/jcu.2018.26.1.40


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
