Impact of a Geometric Correction for Proximal Flow Constraint on the Assessment of Mitral Regurgitation Severity Using the Proximal Flow Convergence Method.
{"title":"Impact of a Geometric Correction for Proximal Flow Constraint on the Assessment of Mitral Regurgitation Severity Using the Proximal Flow Convergence Method.","authors":"Jeong Yoon Jang, Joon-Won Kang, Dong Hyun Yang, Sahmin Lee, Byung Joo Sun, Dae-Hee Kim, Jong-Min Song, Duk-Hyun Kang, Jae-Kwan Song","doi":"10.4250/jcu.2018.26.1.33","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Overestimation of the severity of mitral regurgitation (MR) by the proximal isovelocity surface area (PISA) method has been reported. We sought to test whether angle correction (AC) of the constrained flow field is helpful to eliminate overestimation in patients with eccentric MR.</p><p><strong>Methods: </strong>In a total of 33 patients with MR due to prolapse or flail mitral valve, both echocardiography and cardiac magnetic resonance image (CMR) were performed to calculate regurgitant volume (RV). In addition to RV by conventional PISA (RV<sub>PISA</sub>), convergence angle (α) was measured from 2-dimensional Doppler color flow maps and RV was corrected by multiplying by α/180 (RV<sub>AC</sub>). RV measured by CMR (RV<sub>CMR</sub>) was used as a gold standard, which was calculated by the difference between total stroke volume measured by planimetry of the short axis slices and aortic stroke volume by phase-contrast image.</p><p><strong>Results: </strong>The correlation between RV<sub>CMR</sub> and RV by echocardiography was modest [RV<sub>CMR</sub> vs. RV<sub>PISA</sub> (r = 0.712, <i>p</i> < 0.001) and RV<sub>CMR</sub> vs. RV<sub>AC</sub> (r = 0.766, <i>p</i> < 0.001)]. However, RV<sub>PISA</sub> showed significant overestimation (RV<sub>PISA</sub> - RV<sub>CMR</sub> = 50.6 ± 40.6 mL vs. RV<sub>AC</sub> - RV<sub>CMR</sub> = 7.7 ± 23.4 mL, <i>p</i> < 0.001). The overall accuracy of RV<sub>PISA</sub> for diagnosis of severe MR, defined as RV ≥ 60 mL, was 57.6% (19/33), whereas it increased to 84.8% (28/33) by using RV<sub>AC</sub> (<i>p</i> = 0.028).</p><p><strong>Conclusion: </strong>Conventional PISA method tends to provide falsely large RV in patients with eccentric MR and a simple geometric AC of the proximal constraint flow largely eliminates overestimation.</p>","PeriodicalId":88913,"journal":{"name":"Journal of cardiovascular ultrasound","volume":"26 1","pages":"33-39"},"PeriodicalIF":0.0000,"publicationDate":"2018-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.4250/jcu.2018.26.1.33","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of cardiovascular ultrasound","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4250/jcu.2018.26.1.33","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2018/3/28 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 2
Abstract
Background: Overestimation of the severity of mitral regurgitation (MR) by the proximal isovelocity surface area (PISA) method has been reported. We sought to test whether angle correction (AC) of the constrained flow field is helpful to eliminate overestimation in patients with eccentric MR.
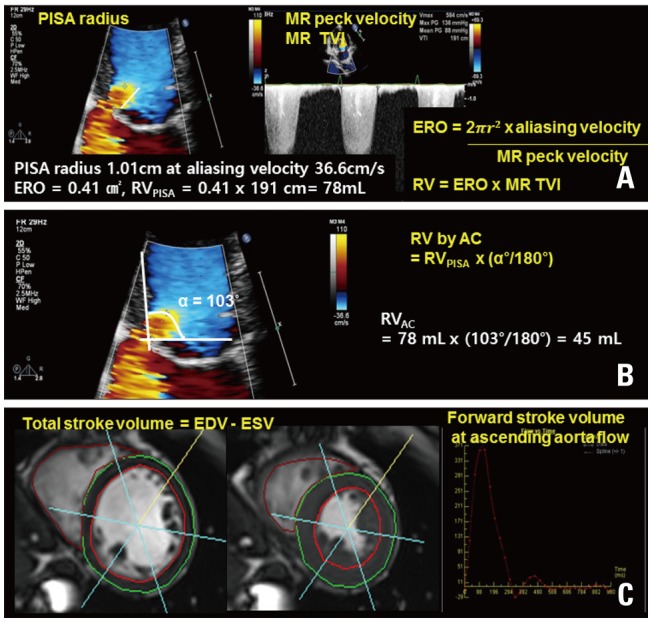
Methods: In a total of 33 patients with MR due to prolapse or flail mitral valve, both echocardiography and cardiac magnetic resonance image (CMR) were performed to calculate regurgitant volume (RV). In addition to RV by conventional PISA (RVPISA), convergence angle (α) was measured from 2-dimensional Doppler color flow maps and RV was corrected by multiplying by α/180 (RVAC). RV measured by CMR (RVCMR) was used as a gold standard, which was calculated by the difference between total stroke volume measured by planimetry of the short axis slices and aortic stroke volume by phase-contrast image.
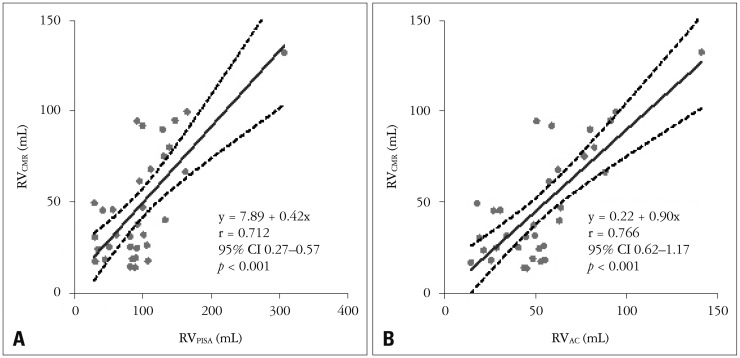
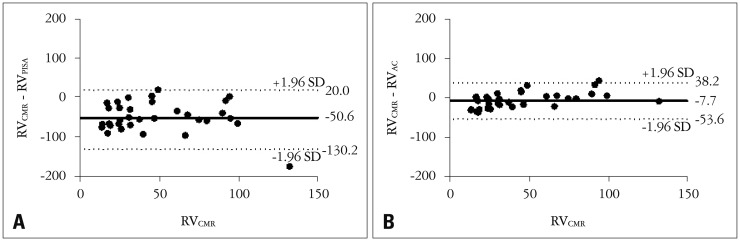
Results: The correlation between RVCMR and RV by echocardiography was modest [RVCMR vs. RVPISA (r = 0.712, p < 0.001) and RVCMR vs. RVAC (r = 0.766, p < 0.001)]. However, RVPISA showed significant overestimation (RVPISA - RVCMR = 50.6 ± 40.6 mL vs. RVAC - RVCMR = 7.7 ± 23.4 mL, p < 0.001). The overall accuracy of RVPISA for diagnosis of severe MR, defined as RV ≥ 60 mL, was 57.6% (19/33), whereas it increased to 84.8% (28/33) by using RVAC (p = 0.028).
Conclusion: Conventional PISA method tends to provide falsely large RV in patients with eccentric MR and a simple geometric AC of the proximal constraint flow largely eliminates overestimation.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
