{"title":"Response to Letter Regarding Article, \"Biventricular Takotsubo Cardiomyopathy Associated with Epilepsy\".","authors":"Ji Yeon Hong","doi":"10.4250/jcu.2016.24.1.88","DOIUrl":null,"url":null,"abstract":"We appreciated the interest of you in our case report.1) Fortunately, we had the previous electrocardiogram (ECG) checked in another hospital 7 years ago, in which there was no Q-waves in leads V1–3 and normal amplitude QRS complexes in limb leads (Fig. 1). Until discharge, we checked the serial ECGs and the ECG of her 2 days of hospitalization started to develop T-wave inversion in leads V5–6 and QT prolongation. The last ECG in our hospital showed persistent low QRS voltages in limb leads and T-wave inversions and QT prolongation in leads V4–6. Also, we found that Q-waves in leads V1–3 lasted despite disappearance of ST segment elevations in V1–3 (Fig. 2). I do not have much clinical experience and have not yet met the patient with recurrent Takotsubo syndrome (TTS) and forme fruste cases of TTS.2) I agree with the idea that the patients with recurrent chest pain and/or dyspnea and normal coronary artery can be diagnosed as TTS. It is not feasible to evaluate the echocardiography as soon as developed chest pain and/or dyspnea, \"smartphone-based technology\" is considered a very useful for diagnosis of unexplained chest pain and/or dyspnea especially in Korea, because Korea is one of the countries with the highest smartphone penetration in the world.3) \n \n \n \nFig. 1 \n \nAn electrocardiogram taken 7 years ago. \n \n \n \n \n \nFig. 2 \n \nAn electrocardiogram obtained before hospital discharge.","PeriodicalId":88913,"journal":{"name":"Journal of cardiovascular ultrasound","volume":"24 1","pages":"88-9"},"PeriodicalIF":0.0000,"publicationDate":"2016-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.4250/jcu.2016.24.1.88","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of cardiovascular ultrasound","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4250/jcu.2016.24.1.88","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2016/3/24 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
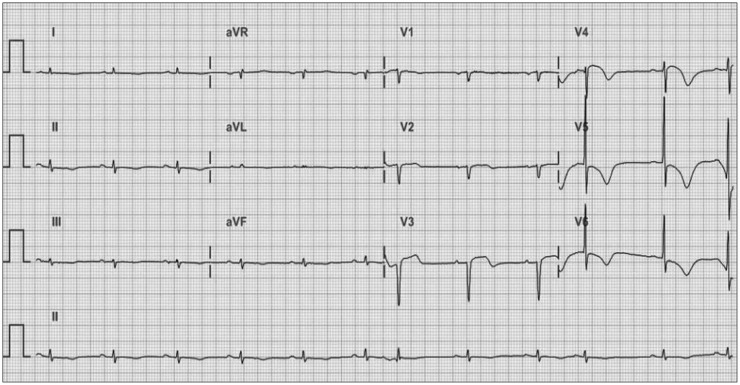
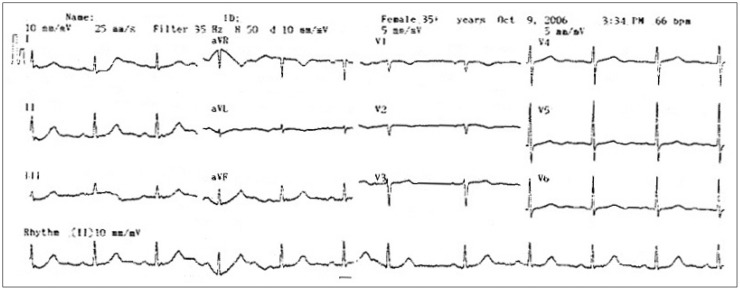
We appreciated the interest of you in our case report.1) Fortunately, we had the previous electrocardiogram (ECG) checked in another hospital 7 years ago, in which there was no Q-waves in leads V1–3 and normal amplitude QRS complexes in limb leads (Fig. 1). Until discharge, we checked the serial ECGs and the ECG of her 2 days of hospitalization started to develop T-wave inversion in leads V5–6 and QT prolongation. The last ECG in our hospital showed persistent low QRS voltages in limb leads and T-wave inversions and QT prolongation in leads V4–6. Also, we found that Q-waves in leads V1–3 lasted despite disappearance of ST segment elevations in V1–3 (Fig. 2). I do not have much clinical experience and have not yet met the patient with recurrent Takotsubo syndrome (TTS) and forme fruste cases of TTS.2) I agree with the idea that the patients with recurrent chest pain and/or dyspnea and normal coronary artery can be diagnosed as TTS. It is not feasible to evaluate the echocardiography as soon as developed chest pain and/or dyspnea, "smartphone-based technology" is considered a very useful for diagnosis of unexplained chest pain and/or dyspnea especially in Korea, because Korea is one of the countries with the highest smartphone penetration in the world.3)
Fig. 1
An electrocardiogram taken 7 years ago.
Fig. 2
An electrocardiogram obtained before hospital discharge.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
