{"title":"Letter Regarding Article, \"Electrocardiogram in a Patient with Takotsubo Syndrome and Cardiogenic Shock\".","authors":"John E Madias","doi":"10.4250/jcu.2016.24.2.179","DOIUrl":null,"url":null,"abstract":"I read with interest the paper by Yoo et al.,1) published in the March, 2016 issue of the Journal, about the 41-year-old previously healthy woman, who suffered Takotsubo syndrome (TTS) complicated by cardiogenic shock, necessitating resuscitation and invasive supportive means of extra-corporeal membrane oxygenation, with eventual full recovery of her heart function. The patient's first electrocardiogram (ECG) (Fig. 1A) recorded on her 2nd visit to the hospital, showed low QRS complexes, in keeping with a recent report,2),3) associating transient attenuation of the ECG QRS complexes (attQRS) and TTS. It is difficult to compare this ECG with the one recorded 1month after discharge (Fig. 1B), since the upper panel of the figure has half of the height of the lower panel, but it appears that there was decrease in QRS voltage in all ECG leads of the admission ECG. This transient attQRS has been attributed to myocardial edema (ME),2) as diagnosed by cardiac magnetic resonance imaging (cMRI).4),5) Unfortunately there was no cMRI in this case, early during the clinical course corresponding to the ECG in Fig. 1A, but much later, a month after admission,1) which of course showed no ME. I will be grateful to the authors if they provide us with information about subsequent ECGs during the patient's follow-up, or ECGs recorded before her admission with TTS (unlikely in a previous healthy young woman), regarding the amplitude of the QRS complexes in those ECGs, in comparison with the ECG of Fig. 1A. \n \n \n \nFig. 1 \n \nElectrocardiographic findings revealed sinus tachycardia with ST segment elevation in precordial leads at initial admission (A) and normalized ST segment on follow up electrocardiogram at 1 month after discharge (B).","PeriodicalId":88913,"journal":{"name":"Journal of cardiovascular ultrasound","volume":"24 2","pages":"179"},"PeriodicalIF":0.0000,"publicationDate":"2016-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.4250/jcu.2016.24.2.179","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of cardiovascular ultrasound","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4250/jcu.2016.24.2.179","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2016/6/22 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
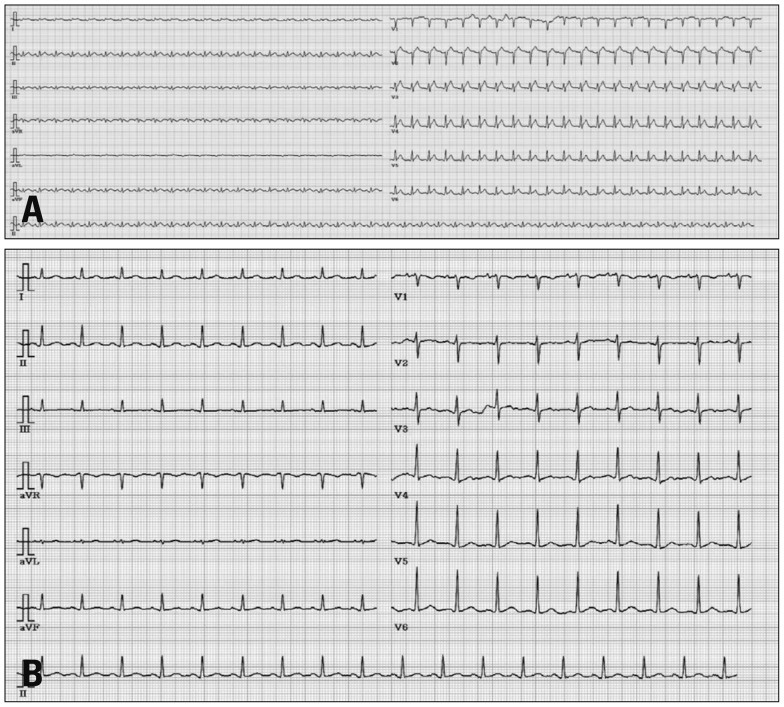
I read with interest the paper by Yoo et al.,1) published in the March, 2016 issue of the Journal, about the 41-year-old previously healthy woman, who suffered Takotsubo syndrome (TTS) complicated by cardiogenic shock, necessitating resuscitation and invasive supportive means of extra-corporeal membrane oxygenation, with eventual full recovery of her heart function. The patient's first electrocardiogram (ECG) (Fig. 1A) recorded on her 2nd visit to the hospital, showed low QRS complexes, in keeping with a recent report,2),3) associating transient attenuation of the ECG QRS complexes (attQRS) and TTS. It is difficult to compare this ECG with the one recorded 1month after discharge (Fig. 1B), since the upper panel of the figure has half of the height of the lower panel, but it appears that there was decrease in QRS voltage in all ECG leads of the admission ECG. This transient attQRS has been attributed to myocardial edema (ME),2) as diagnosed by cardiac magnetic resonance imaging (cMRI).4),5) Unfortunately there was no cMRI in this case, early during the clinical course corresponding to the ECG in Fig. 1A, but much later, a month after admission,1) which of course showed no ME. I will be grateful to the authors if they provide us with information about subsequent ECGs during the patient's follow-up, or ECGs recorded before her admission with TTS (unlikely in a previous healthy young woman), regarding the amplitude of the QRS complexes in those ECGs, in comparison with the ECG of Fig. 1A.
Fig. 1
Electrocardiographic findings revealed sinus tachycardia with ST segment elevation in precordial leads at initial admission (A) and normalized ST segment on follow up electrocardiogram at 1 month after discharge (B).


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
