{"title":"Normal Reference Values for Doppler Echocardiography: Influences of Ageing, Gender and Ethnicity.","authors":"Dong Ryeol Ryu","doi":"10.4250/jcu.2016.24.2.112","DOIUrl":null,"url":null,"abstract":"REFER TO THE PAGE 144-152 \n \nEchocardiography is now considered a standard diagnostic tool that enables the noninvasive quantification of cardiac chamber size, ventricular mass, and systolic function in various clinical situations. Technological progress in Doppler echocardiography has enabled the provision of hemodynamic information and the assessment of valvular heart disease and ventricular diastolic function.1) \n \nWhen interpreting the results of medical tests, comparisons are usually made with a reference range that defines the values seen in health or considered desirable for health, and the effectiveness of any diagnostic test depends on its ability to accurately detect abnormalities. Echocardiography is no exception and it is essential to establish 'normal' reference values for echocardiography.2) \n \nThe population targeted and method used to collect the data are crucial for defining reference values. However, current Doppler echocardiography reference values are derived mainly from North American and European population studies with wide heterogeneity of their inclusion and exclusion criteria and may not be applicable to other populations.3) Reported normal reference values differ according to age, gender, and ethnicity.4),5),6) Several studies have examined these differences. However, the EchoNoRMAL study and an echocardiographic study of Latinos focused mainly on cardiac chamber size,7),8) while Okura et al.9) could not completely exclude subclinical conditions such as diabetes and renal failure that might have changes left ventricular (LV) diastolic parameters. \n \nWith increased awareness of the importance of accounting for age, gender, and ethnicity, several studies have obtained normal reference ranges for Doppler data for specific healthy populations,10),11),12),13) as listed in Table 1. \n \n \n \nTable 1 \n \nStudies that provided normal reference values for variables from Doppler and TDI according to sex and age groups in specific ethnic group \n \n \n \nThe Normal Echocardiographic Measurements in a Korean Population (NORMAL) study is the first Korean multicenter study providing reference values for the most useful Doppler parameters according to age and gender using conventional echocardiographic approaches.14) The NORMAL study ran from January 2011 to March 2014 and included 1003 normal adults (age 20–79 years) who had no significant cardiac disorders or clinical illnesses that might have affected cardiac structure and function, such as hypertension and diabetes. A previous study of normal echocardiographic reference values did not include tissue Doppler imaging (TDI) variables or provide sex-specific reference values.15) \n \nThe NORMAL Doppler study showed that normal ageing is associated with a number of changes in the heart and vascular system. Briefly, the mitral early diastolic inflow velocity (E), late diastolic inflow velocity (A), and E/A ratio were higher in women than in men. There were also considerable differences in the septal and lateral mitral annular velocities, and every TDI variable measured from the lateral annulus was greater compared to the values measured from the septal annulus. However, there were no significant differences in the septal and lateral early diastolic annular velocities (e') between men and women. The septal E/e' value in men was lower than in women. \n \nThe mitral E/A ratio, e' velocity, and E/e', which are representative variables used to evaluate diastolic dysfunction, decrease with age in both men and women. These results have been consistent in studies of European, Japanese, and Chinese populations and confirm that age reference values should be considered when analyzing diastolic function.10),11),12),13),16) These findings might partially explain why elderly people are likely to develop heart failure (HF) with a preserved ejection fraction and higher filling pressure.17) \n \nHowever, in addition to the differences in the E/A ratio, e', and E/e' ratio between men and women among these studies, the changes with age were also not identical. This might be due to ethnicity, relatively small sample sizes, or the age and gender distributions of the study populations. \n \nEthnicity is an important determinant of the cardiovascular adaptation of systolic and diastolic function. Racial and gender differences in large-artery structure and function, endothelial function, the renin-angiotensin system, and levels of vasoactive cytokines may partially explain the differences.18) Also, in the studies mentioned above,10),11),12),13) the study populations ranged from 449 to 1394 and the proportion of males ranged from 44% to 55%. The numbers of participants in the various age groups were different. \n \nAs mentioned above, values of the mitral inflow E, E/A, and E/e' in men were significantly lower than in women, which is consistent with studies in Norwegian and Japanese populations.10),12) This suggests the need for gender-specific reference values in clinical practice. In women, HF is associated more with LV diastolic dysfunction than in men, whereas LV systolic dysfunction is the predominant cause of HF in men.19) Daimon et al.16) reported that for subjects 50 years. Menopause usually occurs at the age of approximately 50 years, and the rapid changes in LV diastolic parameters in women over 50 seem to be consistent with postmenopausal status. The effects of estrogen and postmenopausal status on smooth muscle proliferation20) and vascular function21) may play a role in the gender-based differences in Doppler echocardiographic parameters. \n \nIn this study, patients with significant hypertension and diabetes were excluded based on the medical histories obtained from the study subjects.14) Therefore, patients with subclinical hypertension22) and diabetes mellitus,23) which are associated with diastolic HF, might be included in this study. This could partially contribute to the difference with previous findings.10),11),12),13) \n \nIn conclusion, heightened awareness of the importance of normal reference values according to ethnicity, age, and gender has emphasized the need for age- and gender-specific Doppler reference values for specific populations. In the future, high-quality comparative studies between different ethnicities and studies of the pathophysiologic effects of ethnicity, aging, and sex on Doppler echocardiographic parameters are needed for the correct diagnosis and management of systolic and diastolic dysfunction.","PeriodicalId":88913,"journal":{"name":"Journal of cardiovascular ultrasound","volume":"24 2","pages":"112-4"},"PeriodicalIF":0.0000,"publicationDate":"2016-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.4250/jcu.2016.24.2.112","citationCount":"4","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of cardiovascular ultrasound","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4250/jcu.2016.24.2.112","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2016/6/22 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 4
Abstract
REFER TO THE PAGE 144-152
Echocardiography is now considered a standard diagnostic tool that enables the noninvasive quantification of cardiac chamber size, ventricular mass, and systolic function in various clinical situations. Technological progress in Doppler echocardiography has enabled the provision of hemodynamic information and the assessment of valvular heart disease and ventricular diastolic function.1)
When interpreting the results of medical tests, comparisons are usually made with a reference range that defines the values seen in health or considered desirable for health, and the effectiveness of any diagnostic test depends on its ability to accurately detect abnormalities. Echocardiography is no exception and it is essential to establish 'normal' reference values for echocardiography.2)
The population targeted and method used to collect the data are crucial for defining reference values. However, current Doppler echocardiography reference values are derived mainly from North American and European population studies with wide heterogeneity of their inclusion and exclusion criteria and may not be applicable to other populations.3) Reported normal reference values differ according to age, gender, and ethnicity.4),5),6) Several studies have examined these differences. However, the EchoNoRMAL study and an echocardiographic study of Latinos focused mainly on cardiac chamber size,7),8) while Okura et al.9) could not completely exclude subclinical conditions such as diabetes and renal failure that might have changes left ventricular (LV) diastolic parameters.
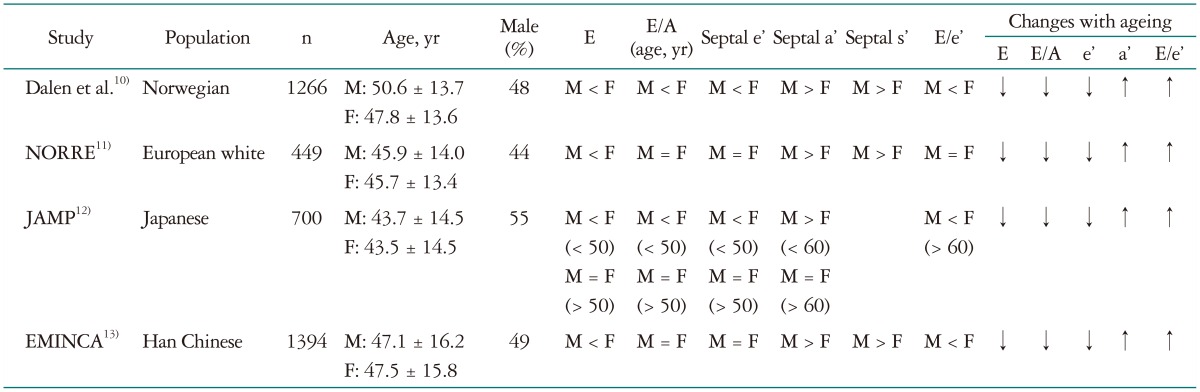
With increased awareness of the importance of accounting for age, gender, and ethnicity, several studies have obtained normal reference ranges for Doppler data for specific healthy populations,10),11),12),13) as listed in Table 1.
Table 1
Studies that provided normal reference values for variables from Doppler and TDI according to sex and age groups in specific ethnic group
The Normal Echocardiographic Measurements in a Korean Population (NORMAL) study is the first Korean multicenter study providing reference values for the most useful Doppler parameters according to age and gender using conventional echocardiographic approaches.14) The NORMAL study ran from January 2011 to March 2014 and included 1003 normal adults (age 20–79 years) who had no significant cardiac disorders or clinical illnesses that might have affected cardiac structure and function, such as hypertension and diabetes. A previous study of normal echocardiographic reference values did not include tissue Doppler imaging (TDI) variables or provide sex-specific reference values.15)
The NORMAL Doppler study showed that normal ageing is associated with a number of changes in the heart and vascular system. Briefly, the mitral early diastolic inflow velocity (E), late diastolic inflow velocity (A), and E/A ratio were higher in women than in men. There were also considerable differences in the septal and lateral mitral annular velocities, and every TDI variable measured from the lateral annulus was greater compared to the values measured from the septal annulus. However, there were no significant differences in the septal and lateral early diastolic annular velocities (e') between men and women. The septal E/e' value in men was lower than in women.
The mitral E/A ratio, e' velocity, and E/e', which are representative variables used to evaluate diastolic dysfunction, decrease with age in both men and women. These results have been consistent in studies of European, Japanese, and Chinese populations and confirm that age reference values should be considered when analyzing diastolic function.10),11),12),13),16) These findings might partially explain why elderly people are likely to develop heart failure (HF) with a preserved ejection fraction and higher filling pressure.17)
However, in addition to the differences in the E/A ratio, e', and E/e' ratio between men and women among these studies, the changes with age were also not identical. This might be due to ethnicity, relatively small sample sizes, or the age and gender distributions of the study populations.
Ethnicity is an important determinant of the cardiovascular adaptation of systolic and diastolic function. Racial and gender differences in large-artery structure and function, endothelial function, the renin-angiotensin system, and levels of vasoactive cytokines may partially explain the differences.18) Also, in the studies mentioned above,10),11),12),13) the study populations ranged from 449 to 1394 and the proportion of males ranged from 44% to 55%. The numbers of participants in the various age groups were different.
As mentioned above, values of the mitral inflow E, E/A, and E/e' in men were significantly lower than in women, which is consistent with studies in Norwegian and Japanese populations.10),12) This suggests the need for gender-specific reference values in clinical practice. In women, HF is associated more with LV diastolic dysfunction than in men, whereas LV systolic dysfunction is the predominant cause of HF in men.19) Daimon et al.16) reported that for subjects 50 years. Menopause usually occurs at the age of approximately 50 years, and the rapid changes in LV diastolic parameters in women over 50 seem to be consistent with postmenopausal status. The effects of estrogen and postmenopausal status on smooth muscle proliferation20) and vascular function21) may play a role in the gender-based differences in Doppler echocardiographic parameters.
In this study, patients with significant hypertension and diabetes were excluded based on the medical histories obtained from the study subjects.14) Therefore, patients with subclinical hypertension22) and diabetes mellitus,23) which are associated with diastolic HF, might be included in this study. This could partially contribute to the difference with previous findings.10),11),12),13)
In conclusion, heightened awareness of the importance of normal reference values according to ethnicity, age, and gender has emphasized the need for age- and gender-specific Doppler reference values for specific populations. In the future, high-quality comparative studies between different ethnicities and studies of the pathophysiologic effects of ethnicity, aging, and sex on Doppler echocardiographic parameters are needed for the correct diagnosis and management of systolic and diastolic dysfunction.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
