{"title":"Bifid Cardiac Apex in an Old Woman.","authors":"Constantina Masoura, Constantina Aggeli, Konstantinos Aznaouridis, Ioannis Felekos, Dimitris Tousoulis","doi":"10.4250/jcu.2017.25.2.70","DOIUrl":null,"url":null,"abstract":"During the embryonic development of the heart, the two ventricles develop as independent structures on the two sides of the primitive plate. Normally, the two ventricles merge together at the apex and their cavities are separated by a bridge formed by muscle fibers (interventricular septum). An apical cardiac notch indicates the developing interventricular septum, and normally disappears later during organogenesis. Bifid cardiac apex arises when this process is abnormal, resulting in a defective union of the two ventricles at the apex and persistence of the cardiac notch. Bifid cardiac apex is a common finding in sea mammals like whales and manatees, however this abnormality is very rare in humans. Only few cases have been reported in the literature, most of which were accompanied by additional congenital cardiac abnormalities. We are presenting the images of a 73-year-old woman with bifid cardiac apex who was admitted in our Department with palpitations, dizziness and diaphoresis. Her past medical history included a transient ischemic attack 5 years ago. Cardiac examination revealed regular rate and rhythm with normal heart sounds, without any murmurs. The systemic physical examination was unremarkable. Chest X-ray was clear with a normal cardiac shillouette. ECG revealed minimal ST-T depression on precordial leads. Ambulatory ECG showed an episode of slow ventricular tachycardia at 105 bpm with a duration of 20 seconds and four shorter ventricular runs. Transthoracic 2D and contrast echocardiography (Fig. 1, Supplementary movie 1, 2, and 3) demonstrated a cleft-like small chamber between the left and right ventricles (bifid left ventricle) with normal systolic function, similar thickness to normal myocardium, and normal perfusion. The right ventricle seemed hypoplastic with adequate systolic function. The atria were of normal size. No additional heart abnormality was detected with echocardiography. Considering the above findings, the lack of a history of coronary artery disease or myocardial infarction, and the abpISSN 1975-4612 / eISSN 2005-9655 Copyright © 2017 Korean Society of Echocardiography www.kse-jcu.org https://doi.org/10.4250/jcu.2017.25.2.70","PeriodicalId":88913,"journal":{"name":"Journal of cardiovascular ultrasound","volume":"25 2","pages":"70-71"},"PeriodicalIF":0.0000,"publicationDate":"2017-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.4250/jcu.2017.25.2.70","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of cardiovascular ultrasound","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4250/jcu.2017.25.2.70","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2017/6/29 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
Abstract
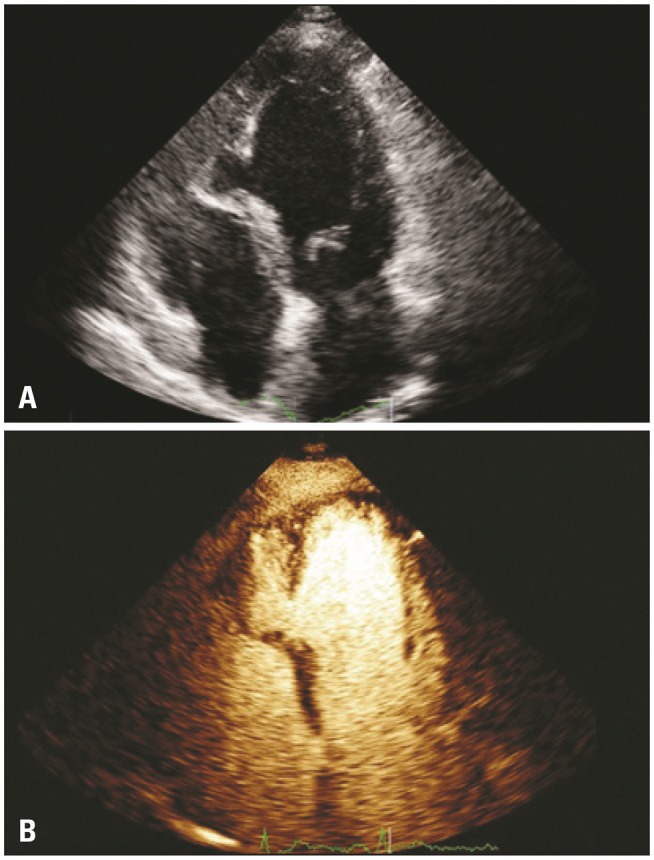
During the embryonic development of the heart, the two ventricles develop as independent structures on the two sides of the primitive plate. Normally, the two ventricles merge together at the apex and their cavities are separated by a bridge formed by muscle fibers (interventricular septum). An apical cardiac notch indicates the developing interventricular septum, and normally disappears later during organogenesis. Bifid cardiac apex arises when this process is abnormal, resulting in a defective union of the two ventricles at the apex and persistence of the cardiac notch. Bifid cardiac apex is a common finding in sea mammals like whales and manatees, however this abnormality is very rare in humans. Only few cases have been reported in the literature, most of which were accompanied by additional congenital cardiac abnormalities. We are presenting the images of a 73-year-old woman with bifid cardiac apex who was admitted in our Department with palpitations, dizziness and diaphoresis. Her past medical history included a transient ischemic attack 5 years ago. Cardiac examination revealed regular rate and rhythm with normal heart sounds, without any murmurs. The systemic physical examination was unremarkable. Chest X-ray was clear with a normal cardiac shillouette. ECG revealed minimal ST-T depression on precordial leads. Ambulatory ECG showed an episode of slow ventricular tachycardia at 105 bpm with a duration of 20 seconds and four shorter ventricular runs. Transthoracic 2D and contrast echocardiography (Fig. 1, Supplementary movie 1, 2, and 3) demonstrated a cleft-like small chamber between the left and right ventricles (bifid left ventricle) with normal systolic function, similar thickness to normal myocardium, and normal perfusion. The right ventricle seemed hypoplastic with adequate systolic function. The atria were of normal size. No additional heart abnormality was detected with echocardiography. Considering the above findings, the lack of a history of coronary artery disease or myocardial infarction, and the abpISSN 1975-4612 / eISSN 2005-9655 Copyright © 2017 Korean Society of Echocardiography www.kse-jcu.org https://doi.org/10.4250/jcu.2017.25.2.70


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
