{"title":"Multimodality Imaging of Anomalous Left Coronary Artery from the Pulmonary Artery.","authors":"Byung Gyu Kim, Sung Woo Cho, Dae Hyun Hwang, Jong Chun Nah","doi":"10.4250/jcu.2017.25.3.107","DOIUrl":null,"url":null,"abstract":"A 22-year-old man was hospitalized for right femur fracture due to a motorcycle accident. Although he had no known cardiac or family history, he felt intermittent chest tightness during moderate intensity of exercise. His electrocardiography showed patterns of left ventricular strain. The echocardiography showed left ventricular hypertrophy, mild eccentric mitral regurgitation, and regional wall motion abnormality and thinning of left anterior descending (LAD) coronary artery territory with lower normal left ventricular systolic function, in which ejection fraction was 50%. Diastolic flow showing peak velocity of 2.5 cm/sec was observed at interventricular septum, which was suspicious of excessive collateral flow at parasternal short axis view (Fig. 1A). Dilated right coronary artery (RCA) ostium of 10 mm was observed (Fig. 1B) on parasternal long axis view, whereas left main coronary artery was not detected in typical situs. Notably, an abnormal retrograde shunt flow was detected (Fig. 1C, Supplementary movie 1) and a drainage site of abnormal shunt flow was observed at the main pulmonary artery (PA) level of parasternal short axis view (Fig. 1D). Thus, we suspected a congenital anomaly of the coronary arteries. Coronary angiography revealed an enlarged and tortuous RCA with abundant septal collateral flows toward the left coronary artery (LCA). An unusual location of the left main coronary artery opening with an abnormal retrograde shunt flow was observed in the left superior part of aorta, most likely PA (Fig. 2A and B, Supplementary movie 2). However, LCA was not shown in the left coronary cusp (Fig. 2C). To specify the location of the left main coronary artery opening, cardiac multidetector computed tomography (CT) was performed and the pISSN 1975-4612 / eISSN 2005-9655 Copyright © 2017 Korean Society of Echocardiography www.kse-jcu.org https://doi.org/10.4250/jcu.2017.25.3.107","PeriodicalId":88913,"journal":{"name":"Journal of cardiovascular ultrasound","volume":"25 3","pages":"107-109"},"PeriodicalIF":0.0000,"publicationDate":"2017-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.4250/jcu.2017.25.3.107","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of cardiovascular ultrasound","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4250/jcu.2017.25.3.107","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2017/9/29 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 2
Abstract
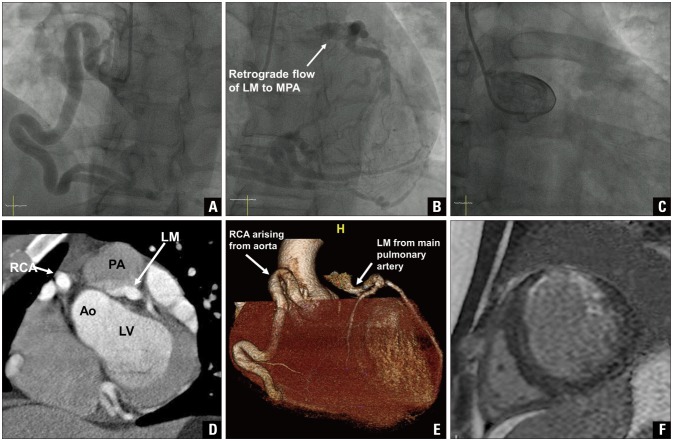
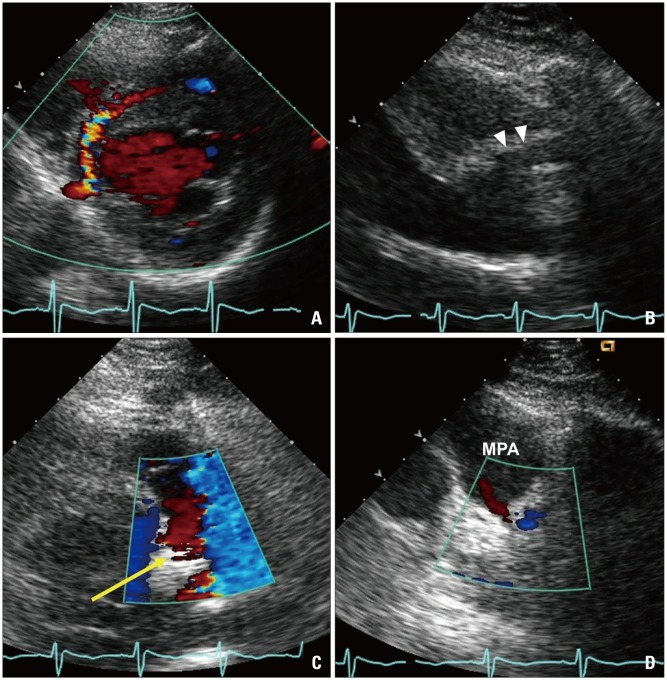
A 22-year-old man was hospitalized for right femur fracture due to a motorcycle accident. Although he had no known cardiac or family history, he felt intermittent chest tightness during moderate intensity of exercise. His electrocardiography showed patterns of left ventricular strain. The echocardiography showed left ventricular hypertrophy, mild eccentric mitral regurgitation, and regional wall motion abnormality and thinning of left anterior descending (LAD) coronary artery territory with lower normal left ventricular systolic function, in which ejection fraction was 50%. Diastolic flow showing peak velocity of 2.5 cm/sec was observed at interventricular septum, which was suspicious of excessive collateral flow at parasternal short axis view (Fig. 1A). Dilated right coronary artery (RCA) ostium of 10 mm was observed (Fig. 1B) on parasternal long axis view, whereas left main coronary artery was not detected in typical situs. Notably, an abnormal retrograde shunt flow was detected (Fig. 1C, Supplementary movie 1) and a drainage site of abnormal shunt flow was observed at the main pulmonary artery (PA) level of parasternal short axis view (Fig. 1D). Thus, we suspected a congenital anomaly of the coronary arteries. Coronary angiography revealed an enlarged and tortuous RCA with abundant septal collateral flows toward the left coronary artery (LCA). An unusual location of the left main coronary artery opening with an abnormal retrograde shunt flow was observed in the left superior part of aorta, most likely PA (Fig. 2A and B, Supplementary movie 2). However, LCA was not shown in the left coronary cusp (Fig. 2C). To specify the location of the left main coronary artery opening, cardiac multidetector computed tomography (CT) was performed and the pISSN 1975-4612 / eISSN 2005-9655 Copyright © 2017 Korean Society of Echocardiography www.kse-jcu.org https://doi.org/10.4250/jcu.2017.25.3.107


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
