{"title":"Treatment Outcomes of Patients with Acute Coronary Syndrome Admitted to Tikur Anbessa Specialized Hospital, Addis Ababa, Ethiopia.","authors":"Kassahun Bogale, Desalew Mekonnen, Teshome Nedi, Minyahil Alebachew Woldu","doi":"10.1177/1179546819839417","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Acute coronary syndrome (ACS) refers to a spectrum of conditions compatible with acute myocardial ischemia and/or infarction that are usually due to an abrupt reduction in coronary blood flow.</p><p><strong>Objective: </strong>The objective of the study was to assess the treatment outcome and associated factors for ACS.</p><p><strong>Methods: </strong>A retrospective cross-sectional study was conducted from January 1, 2012 to December 31, 2014.</p><p><strong>Results: </strong>Of 124 ACS patients who were admitted during the 3 years' period, 90 (72.6%) were diagnosed with ST segment elevation myocardial infarction (STEMI). The mean age was 56.3 ± 13.7 years. The average length of hospital stay was 9.77 ± 6.42 days. The average time from onset of ACS symptoms to presentation in the emergency department was 3.8 days (91.7 hours). In about 76 (61.3%) patients, hypertension was the leading risk factor for development of ACS, and 36.4% of ACS patients were either Killip class III or IV. Biomarkers were measured for 118 (95.2%) patients, and 79.2% of patients had ejection fraction of less than 40% and 29.2% had less than 30%. In-hospital medication use includes loading dose of aspirin (79%), anticoagulants (77.4%), beta blockers (88.1%), statins (85.5%), morphine (12.9%), and nitrates (35.5%). The in-hospital mortality was 27.4%. The predictors for in-hospital mortality were age (<i>P</i> = .042), time from symptom onset to presentation (<i>P</i> = .001), previous history of hypertension (<i>P</i> = .025), being Killip class III and IV (<i>P</i> = .001), and STEMI diagnosis (<i>P</i> = .005).</p><p><strong>Conclusions: </strong>The medical management of ACS patients in Tikur Anbessa Specialized Hospital (TASH) was in line with the recommendations of international guidelines but in-hospital mortality was extremely high (27.4%).</p>","PeriodicalId":10419,"journal":{"name":"Clinical Medicine Insights. Cardiology","volume":"13 ","pages":"1179546819839417"},"PeriodicalIF":3.3000,"publicationDate":"2019-04-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/42/30/10.1177_1179546819839417.PMC6472164.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Medicine Insights. Cardiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/1179546819839417","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2019/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Acute coronary syndrome (ACS) refers to a spectrum of conditions compatible with acute myocardial ischemia and/or infarction that are usually due to an abrupt reduction in coronary blood flow.
Objective: The objective of the study was to assess the treatment outcome and associated factors for ACS.
Methods: A retrospective cross-sectional study was conducted from January 1, 2012 to December 31, 2014.
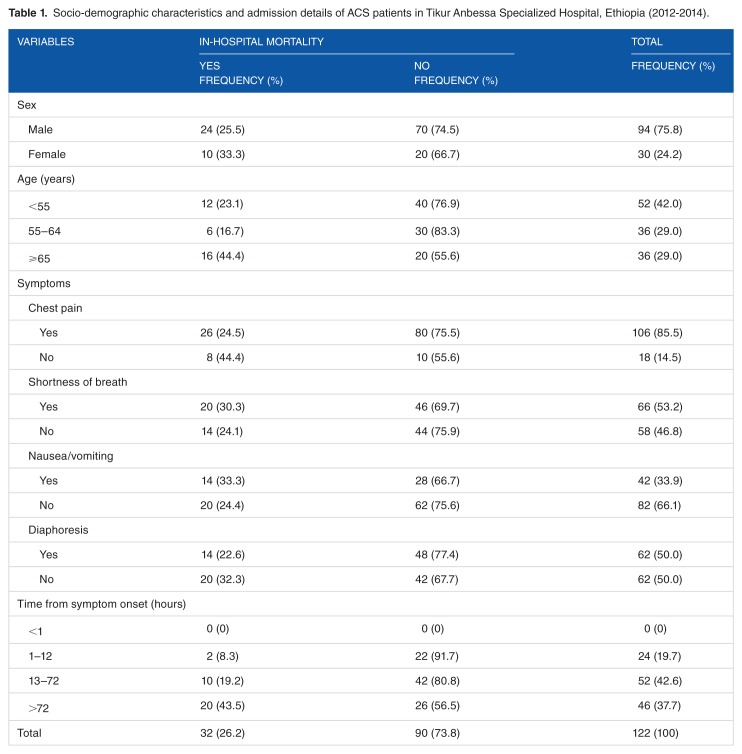
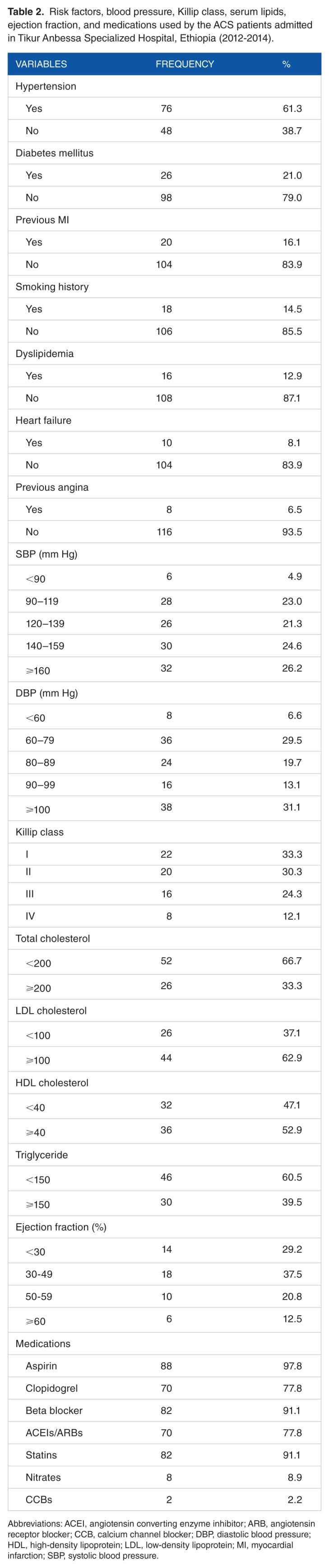
Results: Of 124 ACS patients who were admitted during the 3 years' period, 90 (72.6%) were diagnosed with ST segment elevation myocardial infarction (STEMI). The mean age was 56.3 ± 13.7 years. The average length of hospital stay was 9.77 ± 6.42 days. The average time from onset of ACS symptoms to presentation in the emergency department was 3.8 days (91.7 hours). In about 76 (61.3%) patients, hypertension was the leading risk factor for development of ACS, and 36.4% of ACS patients were either Killip class III or IV. Biomarkers were measured for 118 (95.2%) patients, and 79.2% of patients had ejection fraction of less than 40% and 29.2% had less than 30%. In-hospital medication use includes loading dose of aspirin (79%), anticoagulants (77.4%), beta blockers (88.1%), statins (85.5%), morphine (12.9%), and nitrates (35.5%). The in-hospital mortality was 27.4%. The predictors for in-hospital mortality were age (P = .042), time from symptom onset to presentation (P = .001), previous history of hypertension (P = .025), being Killip class III and IV (P = .001), and STEMI diagnosis (P = .005).
Conclusions: The medical management of ACS patients in Tikur Anbessa Specialized Hospital (TASH) was in line with the recommendations of international guidelines but in-hospital mortality was extremely high (27.4%).




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
