{"title":"Appropriate Blood Pressure in Cerebral Aneurysm Clipping for Prevention of Delayed Ischemic Neurologic Deficits.","authors":"Cattleya Thongrong, Pornthep Kasemsiri, Pichayen Duangthongphon, Amnat Kitkhuandee","doi":"10.1155/2020/6539456","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Delayed ischemic neurologic deficit (DNID) is a problem after cerebral aneurysm clipping. Intraoperative hypotension seems to be indicated as a risk factor, but it remains a controversial issue with varying low-blood pressure levels accepted.</p><p><strong>Methods: </strong>A retrospective, hospital-based, case-control study was performed with patients who received general anesthesia for cerebral aneurysm clipping. 42 medical record charts were randomly selected and matched 1 : 2 (1 case with DNID : 2 controls without DNID) based on the type of general anesthetic techniques and severity of subarachnoid hemorrhage. The optimal cutoff points of hemodynamic response were calculated by the area under the curve.</p><p><strong>Results: </strong>Data suggested that the optimal cutoff points for lowest blood pressure for prevention of DNID should be systolic blood pressure (SBP) of 95 mmHg (sensitivity of 78.6%; specificity of 53.6%), diastolic blood pressure (DBP) of 50 mmHg (sensitivity of 71.4%; specificity of 67.9%), and mean arterial pressure (MAP) of 61.7 mmHg (sensitivity of 85.7%; specificity of 35.7%). Furthermore, the optimal cutoff point mean difference baseline blood pressure was recommended as Δ SBP of 36 mmHg (sensitivity of 85.7%; specificity of 60.7%), Δ DBP of 27 mmHg (sensitivity of 92.9%; specificity of 71.4%), and Δ MAP of 32 mmHg (sensitivity of 92.9%; specificity of 85.7%). No significant difference between DNID and non-DNID groups was found for end-tidal carbon dioxide (ETCO<sub>2</sub>) and has poor diagnostic value for predicting DNID.</p><p><strong>Conclusion: </strong>To prevent DNID, we recommend that optimal blood pressure should not be lower than 95 for SBP, 50 for DBP, and 61.7 mmHg for MAP. Additionally, we suggest that Δ SBP, Δ DBP, and Δ MAP should be less than 36, 27, and 32 mmHg, respectively.</p>","PeriodicalId":7834,"journal":{"name":"Anesthesiology Research and Practice","volume":"2020 ","pages":"6539456"},"PeriodicalIF":1.3000,"publicationDate":"2020-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2020/6539456","citationCount":"5","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Anesthesiology Research and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2020/6539456","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 5
Abstract
Background: Delayed ischemic neurologic deficit (DNID) is a problem after cerebral aneurysm clipping. Intraoperative hypotension seems to be indicated as a risk factor, but it remains a controversial issue with varying low-blood pressure levels accepted.
Methods: A retrospective, hospital-based, case-control study was performed with patients who received general anesthesia for cerebral aneurysm clipping. 42 medical record charts were randomly selected and matched 1 : 2 (1 case with DNID : 2 controls without DNID) based on the type of general anesthetic techniques and severity of subarachnoid hemorrhage. The optimal cutoff points of hemodynamic response were calculated by the area under the curve.
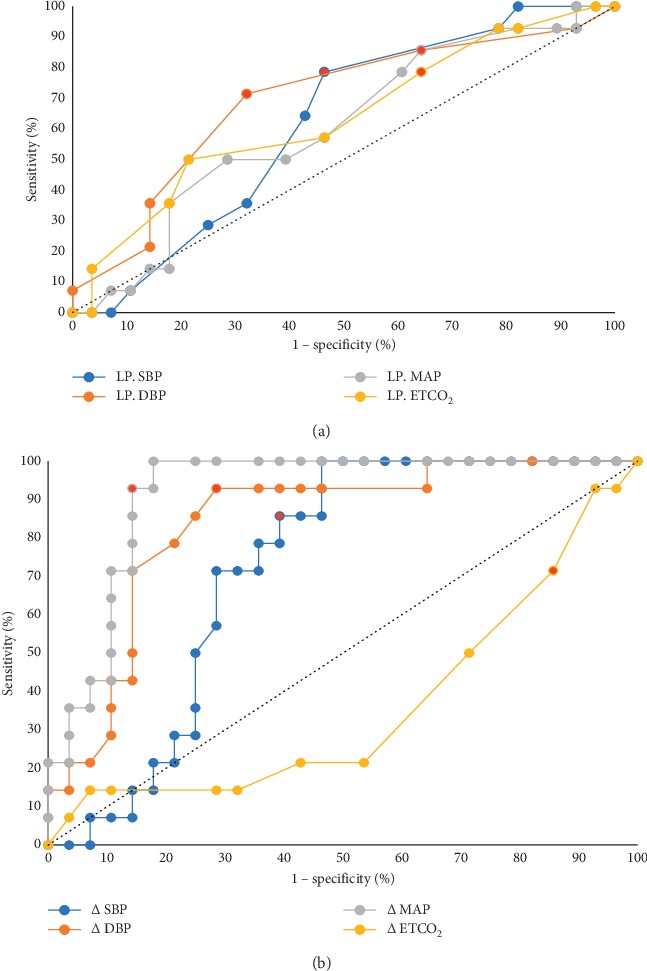
Results: Data suggested that the optimal cutoff points for lowest blood pressure for prevention of DNID should be systolic blood pressure (SBP) of 95 mmHg (sensitivity of 78.6%; specificity of 53.6%), diastolic blood pressure (DBP) of 50 mmHg (sensitivity of 71.4%; specificity of 67.9%), and mean arterial pressure (MAP) of 61.7 mmHg (sensitivity of 85.7%; specificity of 35.7%). Furthermore, the optimal cutoff point mean difference baseline blood pressure was recommended as Δ SBP of 36 mmHg (sensitivity of 85.7%; specificity of 60.7%), Δ DBP of 27 mmHg (sensitivity of 92.9%; specificity of 71.4%), and Δ MAP of 32 mmHg (sensitivity of 92.9%; specificity of 85.7%). No significant difference between DNID and non-DNID groups was found for end-tidal carbon dioxide (ETCO2) and has poor diagnostic value for predicting DNID.
Conclusion: To prevent DNID, we recommend that optimal blood pressure should not be lower than 95 for SBP, 50 for DBP, and 61.7 mmHg for MAP. Additionally, we suggest that Δ SBP, Δ DBP, and Δ MAP should be less than 36, 27, and 32 mmHg, respectively.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
