S Alvarado-Ramos, V J Lara-Díaz, M R López-Gutiérrez, M E Torcida-González, J F Campos-Rodríguez
{"title":"Minimally Invasive Hemodynamic Assessment during Obstetric Hysterectomy for Invasive Placentation with Epidural Anesthesia.","authors":"S Alvarado-Ramos, V J Lara-Díaz, M R López-Gutiérrez, M E Torcida-González, J F Campos-Rodríguez","doi":"10.1155/2020/1968354","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The present study aimed to describe the evolution of hemodynamic parameters over time of patients with invasive placentation during their third trimester who were delivered via cesarean section and subsequently underwent obstetric hysterectomy under epidural anesthesia.</p><p><strong>Methods: </strong>A prospective, descriptive, longitudinal, 11-month cohort study of 43 patients aged between 18 and 37 years who presented with invasive placentation. Minimal invasive monitoring was placed before the administration of epidural anesthesia for hemodynamic parameter tracking during the cesarean section. After delivery, the patients underwent an obstetric hysterectomy. Blood loss, hemodynamic parameters, and coagulation were managed via goal-directed therapy. Parameters were compared via repeated measures ANOVA and effect size estimation (Cohen's d).</p><p><strong>Results: </strong>The mean age of the patients was 29.2 ± 3.4 years and was moderately overweight. They had minor cardiac index variance (<i>P</i>=NS, no significance), vascular systemic resistance index (NS), heart rate (<i>P</i>=NS), and median arterial pressure (<i>P</i>=NS). Differences were observed in the stroke volume index (<i>P</i>=0.015) due to moderately higher values (<i>d</i> = 0.3, <i>P</i>=0.016) in the middle of the surgery. Patients had lower cardiac index (<i>d</i> = -0.36, NS) and cardiac workload requirements (<i>d</i> = -0.29, <i>P</i>=0.034) toward the completion of surgery.</p><p><strong>Conclusion: </strong>Patients who are in their third trimester and who subsequently underwent obstetric hysterectomy under epidural anesthesia had modest surgical hemodynamic variance and reduced cardiac workload requirements toward the end of the surgery.</p>","PeriodicalId":7834,"journal":{"name":"Anesthesiology Research and Practice","volume":"2020 ","pages":"1968354"},"PeriodicalIF":1.3000,"publicationDate":"2020-10-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2020/1968354","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Anesthesiology Research and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2020/1968354","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 1
Abstract
Background: The present study aimed to describe the evolution of hemodynamic parameters over time of patients with invasive placentation during their third trimester who were delivered via cesarean section and subsequently underwent obstetric hysterectomy under epidural anesthesia.
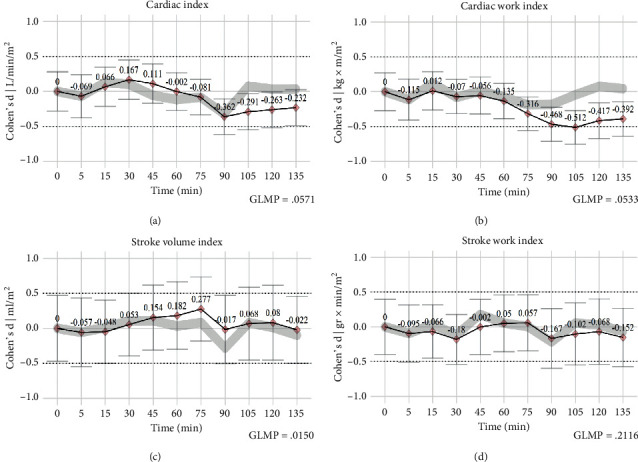
Methods: A prospective, descriptive, longitudinal, 11-month cohort study of 43 patients aged between 18 and 37 years who presented with invasive placentation. Minimal invasive monitoring was placed before the administration of epidural anesthesia for hemodynamic parameter tracking during the cesarean section. After delivery, the patients underwent an obstetric hysterectomy. Blood loss, hemodynamic parameters, and coagulation were managed via goal-directed therapy. Parameters were compared via repeated measures ANOVA and effect size estimation (Cohen's d).
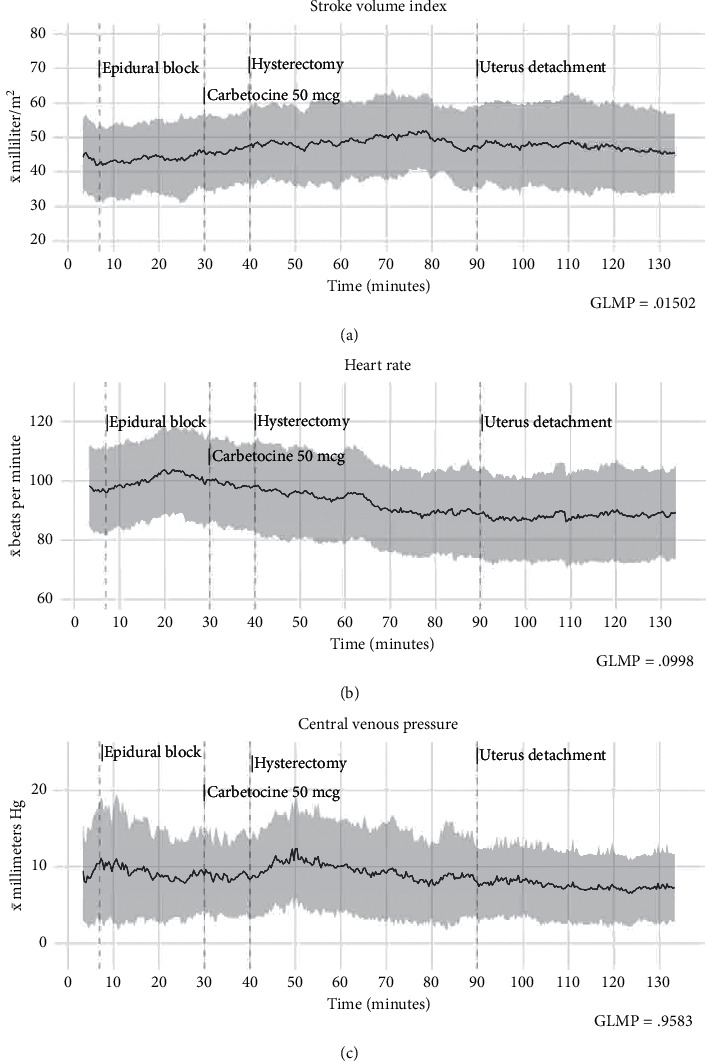
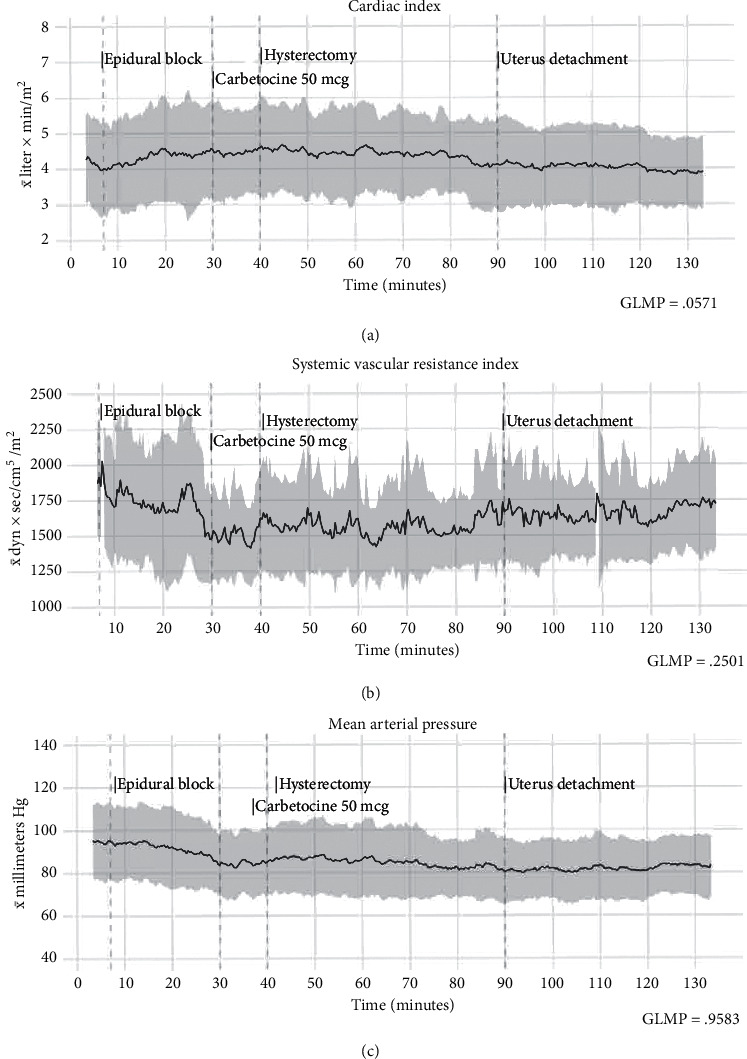
Results: The mean age of the patients was 29.2 ± 3.4 years and was moderately overweight. They had minor cardiac index variance (P=NS, no significance), vascular systemic resistance index (NS), heart rate (P=NS), and median arterial pressure (P=NS). Differences were observed in the stroke volume index (P=0.015) due to moderately higher values (d = 0.3, P=0.016) in the middle of the surgery. Patients had lower cardiac index (d = -0.36, NS) and cardiac workload requirements (d = -0.29, P=0.034) toward the completion of surgery.
Conclusion: Patients who are in their third trimester and who subsequently underwent obstetric hysterectomy under epidural anesthesia had modest surgical hemodynamic variance and reduced cardiac workload requirements toward the end of the surgery.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
