Nicholas M Brown, James F McDonald, Robert A Sershon, Robert H Hopper
{"title":"The Effect of Intraoperative Radiographs on Component Position and Leg Length during Routine Posterior Approach Total Hip Arthroplasty.","authors":"Nicholas M Brown, James F McDonald, Robert A Sershon, Robert H Hopper","doi":"10.5371/hp.2021.33.3.128","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Accurate component placement and restoration of patient anatomy are critical in total hip arthroplasty (THA) surgery. Although intraoperative radiographs are sometimes utilized, it is unclear whether this practice can improve accuracy.</p><p><strong>Materials and methods: </strong>This study evaluated acetabular cup abduction, anteversion, leg length, and offset among 100 posterior approach THAs performed without imaging (No X-ray group) and compared them to a subsequent series of 100 THAs where an intraoperative radiograph was taken with the trial components in place (X-ray group). THAs were performed using a posterior approach by a single, experienced surgeon whose goal was to place the cup at 45° of abduction and 30° of anteversion. Supine anteroposterior pelvic digital radiographs taken at the first (nominal 4-week) postoperative visit were used for measurements.</p><p><strong>Results: </strong>Slight differences in cup abduction (47°±6° vs 44°±6°, respectively, <i>P</i>=0.003) and anteversion angle (35°±6° vs 31°±6°, respectively, <i>P</i><0.001) were observed between the X-ray and No X-ray groups; however, a similar proportion of cups within 10° of the target angles was observed (76% vs 83%, respectively, <i>P</i>=0.22). No difference in offset measurements (1.1±6.6 mm vs 0.3±6.9 mm, respectively, <i>P</i>=0.42) or leg lengths (0.3±3.8 mm vs 0.3±4.8 mm, respectively, <i>P</i>=0.94) was observed between the X-ray and No X-ray groups; however, the X-ray group showed less leg length variation (<i>P</i>=0.05).</p><p><strong>Conclusion: </strong>In this study, the routine use of intraoperative radiographs was not associated with improved implant positioning for uncomplicated primary THA.</p>","PeriodicalId":73239,"journal":{"name":"Hip & pelvis","volume":"33 3","pages":"128-139"},"PeriodicalIF":0.0000,"publicationDate":"2021-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/d0/94/hp-33-128.PMC8440128.pdf","citationCount":"5","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Hip & pelvis","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5371/hp.2021.33.3.128","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/9/6 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 5
Abstract
Purpose: Accurate component placement and restoration of patient anatomy are critical in total hip arthroplasty (THA) surgery. Although intraoperative radiographs are sometimes utilized, it is unclear whether this practice can improve accuracy.
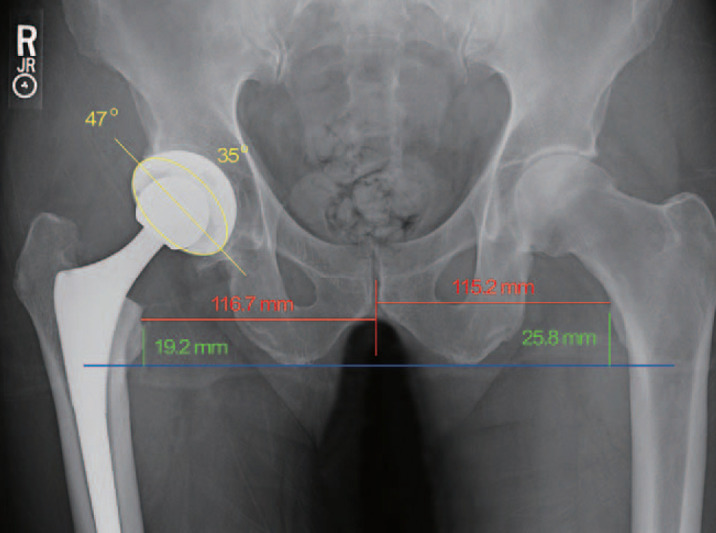
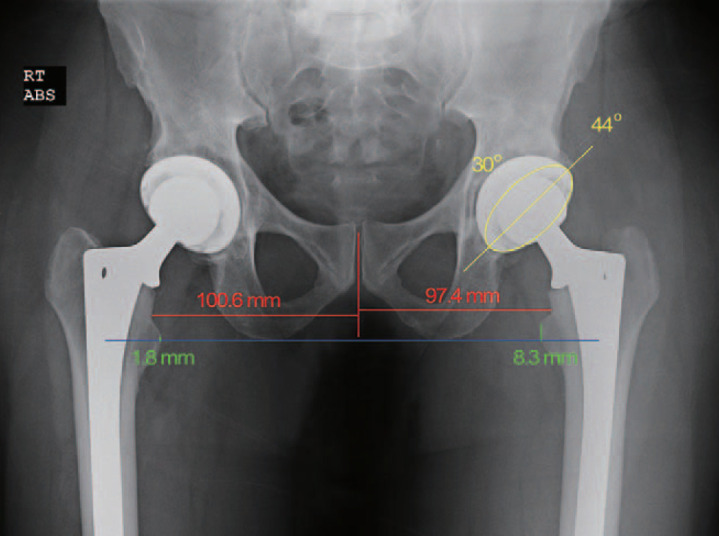
Materials and methods: This study evaluated acetabular cup abduction, anteversion, leg length, and offset among 100 posterior approach THAs performed without imaging (No X-ray group) and compared them to a subsequent series of 100 THAs where an intraoperative radiograph was taken with the trial components in place (X-ray group). THAs were performed using a posterior approach by a single, experienced surgeon whose goal was to place the cup at 45° of abduction and 30° of anteversion. Supine anteroposterior pelvic digital radiographs taken at the first (nominal 4-week) postoperative visit were used for measurements.
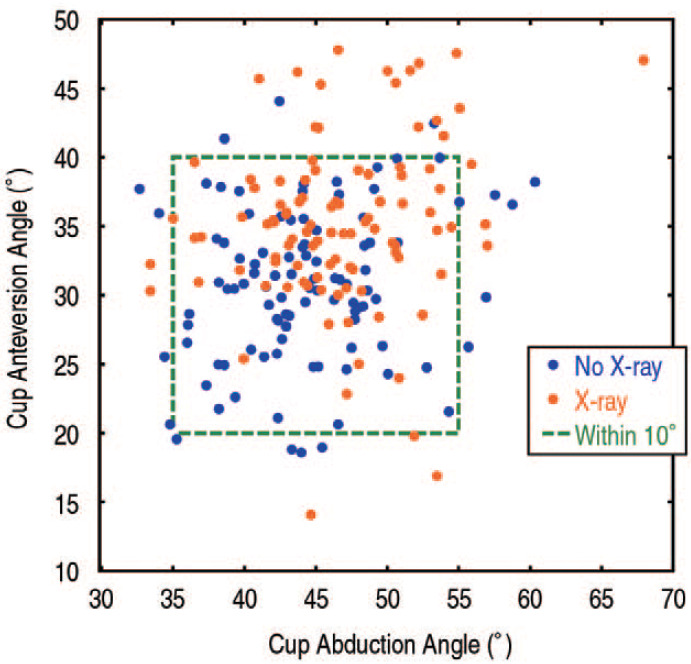
Results: Slight differences in cup abduction (47°±6° vs 44°±6°, respectively, P=0.003) and anteversion angle (35°±6° vs 31°±6°, respectively, P<0.001) were observed between the X-ray and No X-ray groups; however, a similar proportion of cups within 10° of the target angles was observed (76% vs 83%, respectively, P=0.22). No difference in offset measurements (1.1±6.6 mm vs 0.3±6.9 mm, respectively, P=0.42) or leg lengths (0.3±3.8 mm vs 0.3±4.8 mm, respectively, P=0.94) was observed between the X-ray and No X-ray groups; however, the X-ray group showed less leg length variation (P=0.05).
Conclusion: In this study, the routine use of intraoperative radiographs was not associated with improved implant positioning for uncomplicated primary THA.
目的:在全髋关节置换术中,准确的假体放置和患者解剖结构的恢复是至关重要的。虽然术中有时使用x线片,但尚不清楚这种做法是否能提高准确性。材料和方法:本研究评估了100例未经影像学检查的后路tha(无x线组)的髋臼杯外展、前伸、腿长和偏移,并将其与随后的100例tha(术中x线组)进行了比较,其中术中x线片拍摄了试验部件。该手术由一位经验丰富的外科医生通过后路进行,其目标是将关节杯置于外展45°和前倾30°。使用术后第一次(名义4周)就诊时拍摄的仰卧位骨盆正位数字x线片进行测量。结果:杯外展(47°±6°vs 44°±6°,P=0.003)和前倾角(35°±6°vs 31°±6°,PP=0.22)有轻微差异。x线组和无x线组的腿距测量(分别为1.1±6.6 mm vs 0.3±6.9 mm, P=0.42)和腿长(分别为0.3±3.8 mm vs 0.3±4.8 mm, P=0.94)均无差异;x线组腿长变化较小(P=0.05)。结论:在本研究中,对于简单的原发性THA,术中常规使用x线片与改善植入物定位无关。


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
